 I expected he would be familiar with cutting edge treatments in the field - perhaps some that Dr. Hopkins was unaware of. I wanted him to tell me if additional risk was created from the bladder puncture in the first surgery, and what could/should be done about that. I wanted to quiz him about best-case and worst-case scenarios, and I thought he might have information on more than the two options I had heard to date (BCG best case, radical cystectomy worst case).
I expected he would be familiar with cutting edge treatments in the field - perhaps some that Dr. Hopkins was unaware of. I wanted him to tell me if additional risk was created from the bladder puncture in the first surgery, and what could/should be done about that. I wanted to quiz him about best-case and worst-case scenarios, and I thought he might have information on more than the two options I had heard to date (BCG best case, radical cystectomy worst case).The problem with high expectations is that your probability of being disappointed is also high. And so it was with my second opinion. While the doctor was as helpful as he could be, and he took longer than he planned to answer all my questions thoroughly, most of my hopes and expectations were not realized. He had not reviewed my records in detail. He did not personally verify the diagnosis. And most of all, he made it clear that he only supported courses of actions that had been thoroughly tested in controlled environments with sufficient test subjects that were published in peer-reviewed journals. While this is both safe and prudent for him, it limited the information he provided to things that would have been easy for me to research on my own. While I did learn some new and valuable information, it was not worthy of my time investment. So I do not recommend him specifically, and I will refer to him as Dr. X. There's no issue with Dr. X - he is certainly representative of mainstream medical opinion. And therefore there is no reason for you to seek him out rather than a competent physician in your local area. The following is a summary of my consultation with Dr. X on Friday, August 29, which lasted for more than an hour.
Dr. X made a great effort to distinguish between cancer RECURRENCE and cancer PROGRESSION. The most important factor in determining whether to continue with BCG treatments and simple TUR surgeries is whether or
 not the cancer PROGRESSES. If you have read any of my other posts, you know that my cancer has been classified as T1 and Grade 3 (T1-G3). The T score is known as "staging" and it measures PROGRESSION. Grade is the strength/differentiation score. A great summary of bladder cancer basics may be found HERE. Like in golf, low numbers are better than high numbers. So if you have bladder cancer, T1-G1 is a nuisance to deal with for lifetime, but it is very unlikely to progress. If you have anything more, progression (e.g. going from T1 to T2, T3, etc.) is a guessing game. Grade and recurrence are the only tools widely used to judge probability of progression. My G3 is the max bad score you can have, and my chance of PROGRESSION is already high. If RECURRENCE happens quickly, the indicators that the cancer will PROGRESS are maxed out, and the standard treatment is radical cystectomy. Dr. X. flatly stated that radical cystectomy has the single, highest survivability statistics over any other standard treatment. It also has a lot of risk and lifestyle impacts, so most patients (myself included) want very much to avoid it. Next we went into my list of questions.
not the cancer PROGRESSES. If you have read any of my other posts, you know that my cancer has been classified as T1 and Grade 3 (T1-G3). The T score is known as "staging" and it measures PROGRESSION. Grade is the strength/differentiation score. A great summary of bladder cancer basics may be found HERE. Like in golf, low numbers are better than high numbers. So if you have bladder cancer, T1-G1 is a nuisance to deal with for lifetime, but it is very unlikely to progress. If you have anything more, progression (e.g. going from T1 to T2, T3, etc.) is a guessing game. Grade and recurrence are the only tools widely used to judge probability of progression. My G3 is the max bad score you can have, and my chance of PROGRESSION is already high. If RECURRENCE happens quickly, the indicators that the cancer will PROGRESS are maxed out, and the standard treatment is radical cystectomy. Dr. X. flatly stated that radical cystectomy has the single, highest survivability statistics over any other standard treatment. It also has a lot of risk and lifestyle impacts, so most patients (myself included) want very much to avoid it. Next we went into my list of questions.Do you concur with the grading and staging of my cancer?
Yes.Did you look at the reports, slide images, or both?
My staff usually looks at the most detailed data they can get. I'm not sure if they were able to get the slide images for you or not.
Do you concur with the diagnosis and recommended course of treatment?
Yes.Were any additional risks added from the bladder perforation during my first TURBT?
Theoretically there is a small risk, but nothing has ever been proved to propagate from a perforation. So I don't believe there is any real additional risk.Would any additional diagnostics be useful?
The only thing you can do is another CT scan.That would only work after something got big enough to be a problem, correct?
Correct.What about an exploratory surgery?
You could not see anything that way until it got big enough to see visually, so it's no better than the CT scan. And nobody would do it.The radiology report from my CT scan indicated inflammation possible outside the bladder and/or in the transverse colon. Is there a probability or risk of abdominal or lymphatic cancer already in progress?
You would have to ask a gastrointestinal doctor for specifics, but I find it doubtful.How would it be diagnosed?
Via colonoscopy.I'm scheduled to get my first one of those next summer after I turn 50. Do you believe the report suggests I should get one sooner?
No, that should not be necessary. Again, you could ask a GI doctor. (Looks like a question for Dr. Chuck)
I have heard that cancer does not like oxygen. My house is at about a mile elevation. Is that a concern? Should I consider supplemental oxygen?
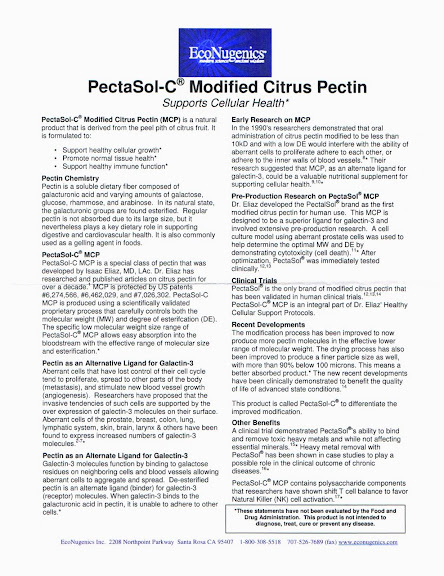
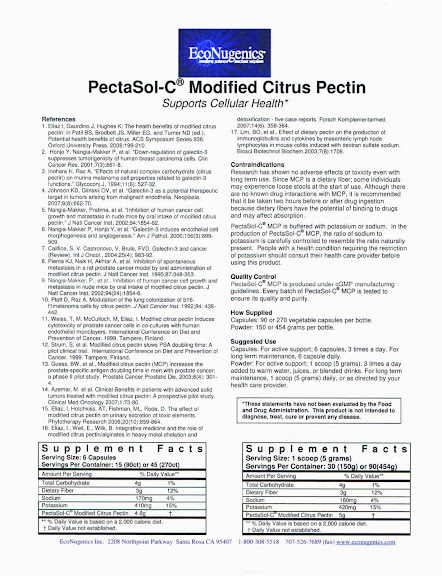
No. Not at all.Do you have an opinion on complementary therapies in addition to the BCG, such as vitamins, MCP, hyperthermia, hyperbaric, or others?
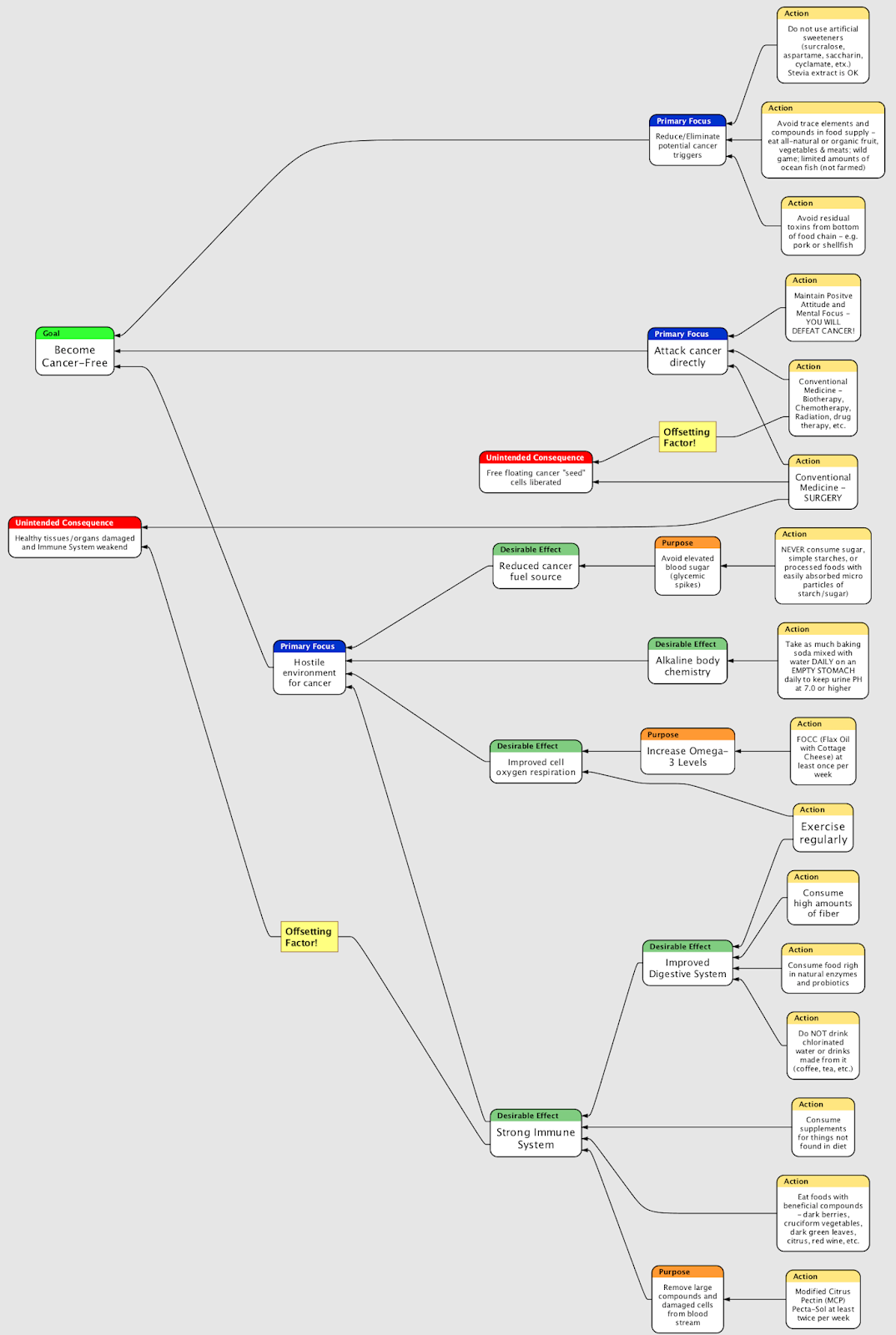
Nothing has been proven to my satisfaction to be helpful. Of course, any of these things COULD help, along with Taxol or other stuff from the Amazon rain forest. There would be an underlying chemical basis, and that would need to be studied and tested under controlled conditions. Just make sure that anything you try won't hurt you, and it's possible that some of it might help.What about specific dietary restrictions, such as avoiding sugar, or a radical change?
Won't matter. You already have cancer and nothing in diet can change that. Diet MIGHT help someone avoid getting cancer, but once you've got it, you've got it. (NOTE: I do not agree with Dr. X on this subject)So there's really NOTHING I can do in addition to the BCG to improve my odds?
I doubt it. I think you're doing everything you can. Just make sure you don't try anything that might hurt.Did you read the information about Oncovite or MCP in my materials?
No.What are my odds at this point?
We have to segregate your RECURRENCE odds from your PROGRESSION odds. Your odds of PROGRESSION are 50%. Your odds of recurrence are significantly higher than that. Early recurrence for your grade (G3) is a strong indicator for progression.How long before the recurrence is not considered "early" and we can go back to TURBT to remove it?
I'd say a year to two years. I really like that one-year threshold, myself. I'd go back to TUR for a patient who had no recurrence for a year, unless there's evidence of progression.Can't progression only be evaluated through resection and lab work?
Often you can tell with the cystoscope.Do you recommend any other diagnostics?
Urine cytology also.I'm also doing a consultation with Dr. Lamm. Are you familiar with him and his work?
Yes, very much so. He and Dr.(I missed the name) pioneered BCG treatments, and his paper in the late 90s documented the effectiveness of maintenance therapy.
Do you have a recommended BCG regimen?
I generally do six doses, and occasionally do maintenance.
Why don't you always do maintenance, if the paper documented the effectiveness?
Because only six patients were able to tolerate the maintenance treatments to their conclusion, I think two or three years. So while the initial sample was big, the end sample was small.
Dr. Lamm has done some recent work with reduced dosages and increased frequency to improve tolerance by patients. Do you have any opinions about that?
If you are doing a consult with Dr. Lamm, you should follow his recommendations for your specific case to the letter. He knows more about it than either Dr. Hopkins or myself. I'd like to know what he recommends for my own education. (I agreed to email him the summary.)
If radical cystectomy is indicated after my October 23 cystoscope, how long do I have to arrange for it and get it done?

If progression is observed, I'd do it immediately. I'd like you on the operating table within six weeks. If not, maybe two to three months. Say 90 days maximum.
If radical cystectomy is indicated, does that always mean taking multiple organs out like prostate, lymph nodes, etc.?
Yes. The cystectomy is really a misnomer. We will take out your bladder, your prostate, and several lymph nodes.What about not taking the "yard sale" approach?
It's not safe. Nobody in the US would perform such a surgery. You should really not focus on this outcome. A positive attitude is going to be very helpful for your upcoming treatments.I agree. But with potentially only six weeks to get it done in the worst case, that would not leave much time to get educated, choose a physician, get the workups, etc.
That's a good point.I read that there's a 2% chance of dying on the table.
It used to be 3% but it's down to 1% now that you won't leave the hospital.I have read that 30% of prostatectomy patients die within 5 years.
That's not accurate at all. I don't know the number, but it's small, like 2-3%.I have also read that 90% of prostatectomy patients lose their "recreational facilities" forever.
Count on it. And count on a 5-10% chance of daytime incontinence and a 15-20% chance of nighttime incontinence. On the other end of the scale there's a 20% chance of needing to do self-catheterizations.What about "nerve sparing" techniques?
Maybe there are some small improvements in this field. I'm not familiar.Any pouch or neobladder techniques better than others?
Most common is the Studer. USC uses T-pouches. I'm not aware of any significant advantages or drawbacks to any one procedure.Any surgeons you would recommend for the radical cycstectomy?
Bernie Bochner at Memorial Sloan-Kettering in Manhattan, Don Skinner at USC in Los Angeles (retired in 2017), or Seth Lerner at Baylor in Houston. I can get you a referral for Bochner if you need it.What's your final summary of my prognosis?
We know certain things that work. BCG works sometimes, but we don't know the exact mechanism. Maintenance therapy works. Removing the prostate and lymph nodes in addition to the bladder works. Radical cystectomy provides the absolute highest chances of survival. Do whatever Lamm recommends for BCG for your specific case. You are doing everything you can (and more) to improve your chances. Keep a positive attitude.Thank you for your time.
Obviously this is a lot to process. My original plan was to stay positive and focus on a positive outcome for October. I had assumed there would be ample time to research the flip side and/or try other therapies if the news is bad. Now I will have to learn more about the bad outcome while staying focused on the positive one. I hope that my session (via phone) with Dr. Lamm is more encouraging.



{kind=link}
{kind=link}
{kind=link}
7 comments:
WOW! That is a lot to take in. Keep a positive attitude and remember you are being prayed for by many people. Thanks for the update.
Denise
Hi Steve, I had the same grading and the BCG knocked back the CIS to pre-cancerous, then another lot of BCG to no-anomalies (why don't they speak English?) and I'm on maintenance as you know with a clear this time.
I think that this lot will make 24 of them I've had in total so that was two lots of 6 and two lots of maintenance (3 then 9 weeks off and another 3).
I really hope that the BCGs have worked for you as they did for me. You keep sticking at it and congratulations on your blog it is a great read.
I didn't realise they punctured your bladder, they did say to me that was a possibility.
Thanks Denise!
And hello ADR. I was very pleased to read your comment here. It's the first time I've heard that they can actually observe the cancer regressing via the scope. I had always felt it was all clean & do BCG, or something/anything there and you go get big surgery - and then they remove a jumble sale's worth of organs & tissues.
So thanks much for the new inputs. It will help me to visualize the BCG at work, and as such will be good biofeedback to help it do its stuff!
Steve, you are quickly becoming an expert on this subject aren't you! That is a lot of information, so what's the bottom line? Do you just wait until the next examine? It sounds like you are doing everything possible to help yourself. I do believe dietary changes can help and they certainly won't hurt. Have you explored any homeopathic treatments or physicians? I have heard of and seen remarkable results from this field.
Thanks Kathie!
Wait and see is the official medical position - Judgment Day on October 23. In the meantime diet is a go, and next target is to work in some reasonable exercise (yuck). Homeopathy is further down the list for now.
Steve, you and I have more in common than bladder cancer and personal distaste for smoking. My parents were heavy smokers too. Have you seen the result of the research at this link: http://info.cancerresearchuk.org/news/archive/pressreleases/2006/november/241084?
Tex
Hi Tex,
I had not seen that article. It suggests secondhand smoke is a bladder cancer precursor. Maybe so. But nothing to do about it at this late date!
Post a Comment