
New country, new doctor, new protocol, new (to me) procedures, same old VERY GOOD result - ALL CLEAR now 14 years and counting! This all happened a couple of weeks ago, and the process was unusual and anticlimactic and did not really feel "real" at the time. But now it does, and I'm pleased to have something unusual to report.
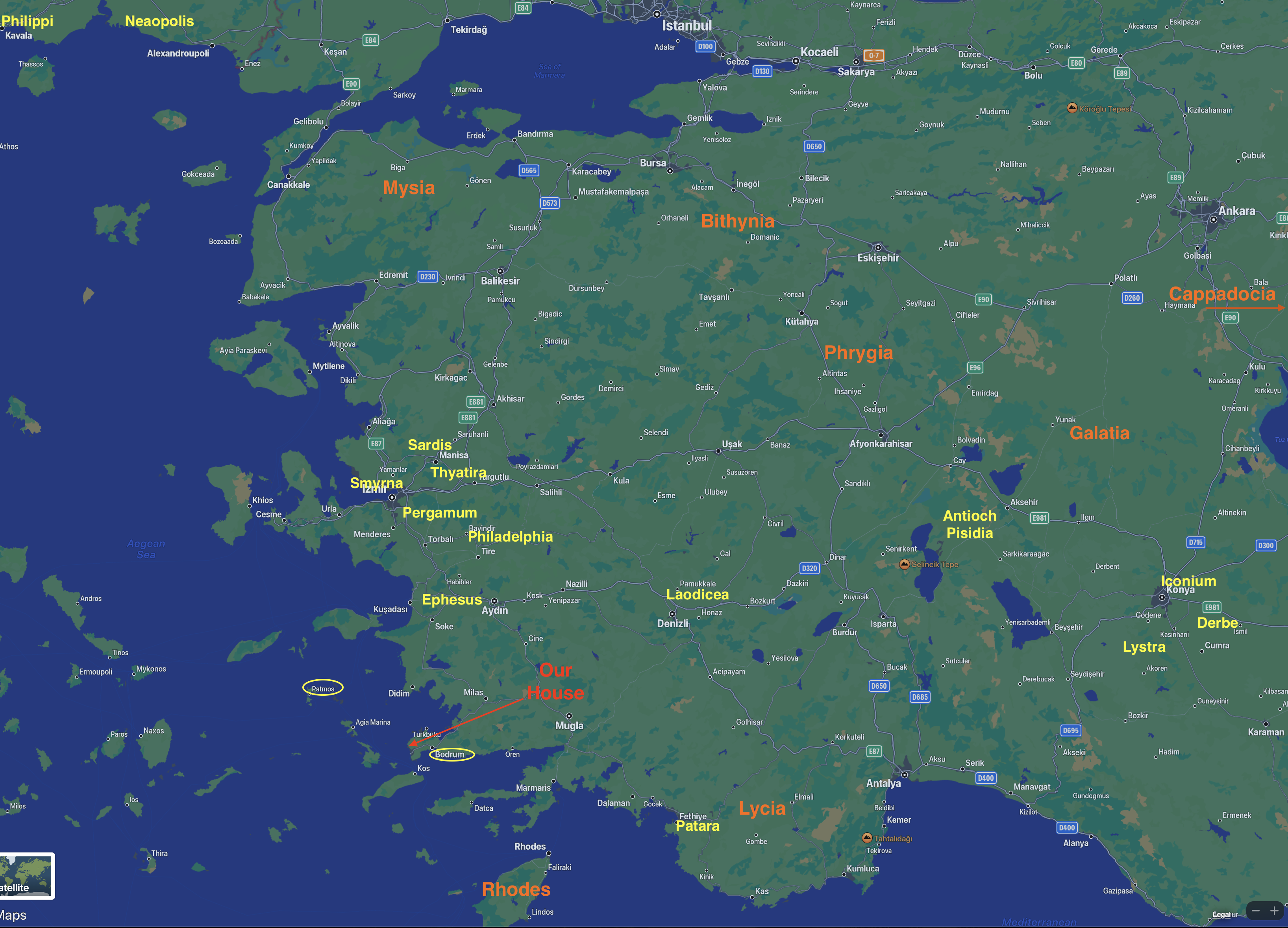
From my last post you will have learned that we decided to retire and have now relocated permanently to Bodrum, Türkiye. That makes chasing Dr. Hopkins (who has moved back to Salt Lake City from Oregon) a bit more expensive and troublesome. Medical and dental care in Türkiye are world class. It is the number one international medical tourism for male hair implants, top 5 for elective cosmetic surgeries, and top 10 for dentistry - the latter being very popular for folks from the UK, who vacation here often. We live in the cosmopolitan area of Bodrum with an enormous summer tourist presence and a very strong year-round international presence, so the demand for excellent healthcare (and other consumer items) is supplied in surplus by enterprising Turkish and international businesses.


Dr. Mirze (in Turkey the docs go by first names) was very interested in the history and documentation I had brought with me, all in English. We started with the date of diagnosis and staging, and he expressed deep concern at the grade of my cancer (T1G3). He asked about follow-up BCG, and I told him first about the Mytomycin chemo-bake following my second TURBT, which he understood. Then I gave him a copy of my spreadsheet that showed every exam, DRE, CT-Scan, and BCG series for the past 13 years. He asked several questions about BCG and was surprised that I had consulted with Dr. Lamm himself. I also gave him the summary of my CT scan last year, 10 years of blood work history, and some recent weight and blood pressure data. He was pleased to have all of it, and even more pleased that I had made copies he could keep. He asked (via Becky) if my PSA values were Total PSA or Free PSA, and was surprised they were Total. I added they are low, and he agreed VERY low. After perusing everything in depth, he said something very excitedly to Becky and showed her a paperback large-format book, all in Turkish. Becky explained, "Dr. Mirze is extremely impressed with the history and level of care your case has been given. He described it as extraordinary, and he also wanted you to know that he is both and expert and advocate of maintenance BCG. The book he showed us was his Doctoral thesis on BCG treatments." I mentioned also the Mytomycin bake, and he agreed, saying it was his standard protocol.
 |
| Cooler than Sickbay on Starship Enterprise! |
Then she sent me on my own to the lab to have blood drawn and urine collected, which went very smoothly, after which I was free to go, and so I departed to my car. On the drive back home Becky did call and told me the cysto would cost just over US$3000. Shocked, I told her to cancel it. She was surprised and asked how much it was in the US. I explained that it was probably more, but that after insurance I paid around US$1000. She said she would double check with the doctor. A few minutes later she called to let me know that the $3k price was given to her by the admin department for a full operating room, general anesthesia, an anesthesiologist, surgical intern, both hard and flexible cystoscopy, and ability to do biopsies. But as the doc told her I needed only a flexible scope, most of that did not apply - but it would still be done in the surgical theater, and the real price would be around US$1300.
By this time I had already decided the doc's exam was good enough, and I was cancer free, and so spending as much as I would in the US or more seemed like a waste of vacationing money. And let's face it - once you decide NOT to do a scope, it's really hard to reverse that decision. I told her to cancel anyway and thanked he for her help. She was quite surprised, but accepted my decision. If the price had come in at the $300-$600 I had expected, I probably would have done it. But now I think I can accept going to every second year for cysto, and that gives me time to see if alternative providers can do cystos in the office rather than in a surgical theater, perhaps bringing the cost way down.
Upon arriving home, I was a bit surprised to see my blood work and urine cytology reports, along with the doctor's full report, were live online for me to see and download - all in English. And the urine culture results arrived 24 hours later. All results were negative or within limits, and PSA still below 1.0. Good news all around. But the bottom line is my logic told me all was good and I am Cancer Free, but not having the experience of SEEING it real-time in living color on a big TV made the entire thing anticlimactic. Now 2 weeks later it feels more real, and I guess I can live without the excitement. Life is good, God is good, and I am super happy with this year's adventure.







































{kind=link}
{kind=link}
{kind=link}
{kind=link}