skip to main |
skip to sidebar
No medical news unless you count having a great time in Acapulco, Guerrereo, Mexico this week. We took a private tour yesterday and saw spectacular city views, had a great lunch, and even saw the famous cliff divers. As dated and touristy as it was, these guys were still impressive to even the most jaded viewer. Prices for most things are low and all the locals are very friendly and glad to see us in the off season. Beer (cerveza) and tequila (El Jimador) consumption have been pretty high, and the weather has been awesome - upper 80s during the day and mid 70s at night. Rain has been pretty much limited to the evenings. Very tropical and muggy. Here are a few pictures to look at. Click on any one for an enormous version.

.

 My friend Kathie wrote a comment on the Dr. Lamm post and referred to a book by another doctor (David Servan-Schreiber) that supports the diet/exercise regimen for battling cancer. Anti-Cancer: A New Way of Life describes some lifestyle changes that can be effective in keeping cancer in remission. I looked at the link and read some previews from the book both there and on Amazon. After only a few months of research on the general topic of cancer and the specific topic of bladder cancer, I have found that there are five options frequently found when searching the internet (or other areas) for adjunct or alternative therapies for cancer treatment.
My friend Kathie wrote a comment on the Dr. Lamm post and referred to a book by another doctor (David Servan-Schreiber) that supports the diet/exercise regimen for battling cancer. Anti-Cancer: A New Way of Life describes some lifestyle changes that can be effective in keeping cancer in remission. I looked at the link and read some previews from the book both there and on Amazon. After only a few months of research on the general topic of cancer and the specific topic of bladder cancer, I have found that there are five options frequently found when searching the internet (or other areas) for adjunct or alternative therapies for cancer treatment.
1) Secret Cure Banned By Doctors - SEND MONEY NOW!!!!!!!!!!!!!!!!!
2) Special vitamin/pill/powder/elixir/liquid from Amazon Rain Forest/China/Tibet/Europe/etc. cures cancer!
3) Get your colonics here! Coffee/filtered water/flower petals/etc. Secret cancer wonder cure is hiding right up your ass!
4) Exercise more you lazy bastard!
5) Change your diet - Western diets, particularly American diets, are BAD BAD BAD!!!
Here is MY OPINION:
Category 1 - SECRET BANNED CURES - This group is entirely populated by scumbags and lowlifes who prey on people's hopes and fears. They should all burn in hell. Trust me - if I found the secret cure for cancer, I would post it on this blog and everywhere else that I could think of FOR FREE. No cancer patient who discovered the "magic cure" would first think, "I have to keep this a secret, and then charge $19.99 for a poorly produced photocopy full of misspelled words (plus shipping and handling)!" Only the lowest of the low would employ this tactic. So don't even waste your time and money.
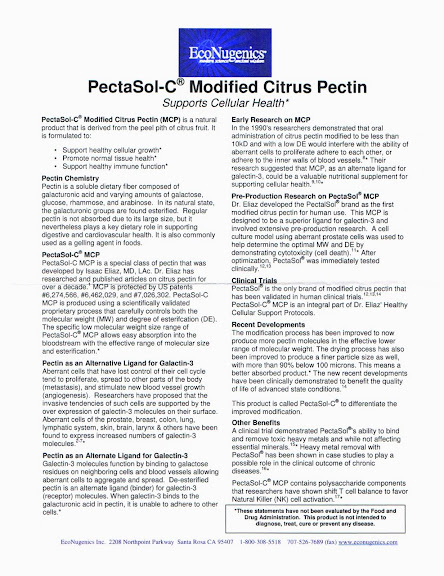
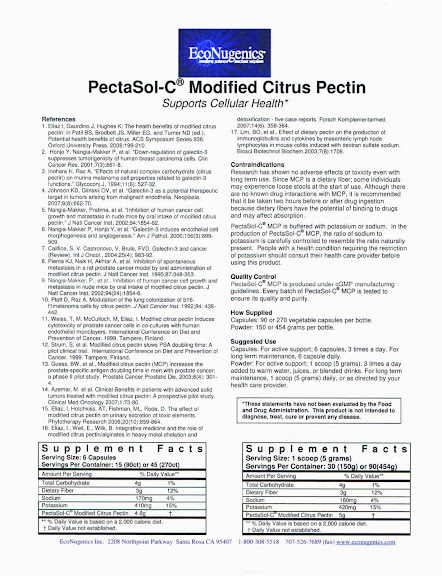
Category 2 - SPECIAL NEW DISCOVERIES - Even the most cynical of doctors (like Dr. X) will admit that SOME of these things might some day prove effective at battling cancer. In the meantime it's a guessing game which, if any, of these might help you out. Dr. Hopkins and Dr. X both advised that you can try any of these things, after assuring yourself that they won't hurt you. And certainly BELIEVING that the special cure COULD help will bring self-healing benefits, and that fact has been scientifically proved to everyone's satisfaction. So if it sounds good, you can afford it, and it won't poison you, go for it! My particular choice is PectaSol-C.
Category 3 - COLONICS - The theory here is that the large intestine is the source of the problem, and it needs exercise and cleaning. While there is some underlying evidence that such things might help, this addresses only the "tail end" of the system, pardon the pun! I wonder if this therapy addresses a symptom rather than a cause. If you are into that sort of thing - go for it. Such treatments are very popular in Europe and becoming more popular in the US, especially in the north of the country. I have no idea why. Certainly if these simple treatments (which can be as often as daily for a while) cured cancer, there's enough people doing them to prove it. So while they may help, there's probably more that can be done. I find the whole idea unappealing. But that's just me...
Category 4 - EXERCISE - It is indisputable that exercise improves everything. But like colonics, it can't be the ONLY thing that works. Plenty of healthy, in-shape people get cancer. So again there's probably more that can be done, and somewhere else to start.
Category 5 - DIET - This is the topic for the post. Back to the doctor and book that Kathie mentioned in her comment. Here's an excerpt from the book's introduction:
If cancer was transmitted essentially through genes, the cancer rate among adopted children would be the same as that among their biological—not their adoptive—parents. In Denmark, where a detailed genetic register traces each individual’s origins, researchers have found the biological parents of more than a thousand children adopted at birth. The researchers’ conclusion, published in the prestigious New England Journal of Medicine, forces us to changes all our assumptions about cancer. They found that the genes of biological parents who died of cancer before fifty had no influence on an adoptee’s risk of developing cancer. On the other hand, death from cancer before the age of fifty of an adoptive parent (who passes on habits but not genes) increased the rate of mortality from cancer fivefold among the adoptees. This study shows that lifestyle is fundamentally involved in vulnerability to cancer. All research on cancer concurs: Genetic factors contribute to at most 15 percent of mortalities from cancer. In short, there is no genetic fatality. We can all learn to protect ourselves.
This is a fascinating line of reasoning. Every human being has cancer pre-factors present in their body, and ONE IN THREE get some form of cancer in their lifetime. Some are deadly, others not. Yet two in three do not. Genetics has been assumed to be a big cancer precursor. If your parents got cancer, you are at higher risk. But you share more than genetics with your parents - you also share environment plus dietary and cultural habits. And plenty of evidence abounds that Europeans and Americans get cancer at a much higher rate than Asians. So race is presumed to be a factor. Yet diet is also a discriminator between these populations. The study mentioned above finds that adopted people got cancer at higher rates if their parents (to whom they were not related at all) died of cancer. Such a finding suggests that environmental factors (such as diet, exposure to toxins, pollutants, radiation, etc.) are stronger cancer precursors than genetics or race. I believe that we must consider diet may be the single biggest contributor to cancer triggers, and therefore to cancer avoidance. And this is exactly what Dr. Lamm was talking about!
You can purchase this book for less than $20 from Amazon by clicking THIS LINK.  The Amazon review links indicate that it's good for self-attitude and general food
The Amazon review links indicate that it's good for self-attitude and general food  guidelines, but sparse on specifics - like just how much of food X should be eaten per day or week. I went ahead and ordered it anyway. And I also ordered a second book, Foods to Fight Cancer: Essential Foods to Help Prevent Cancer, by Richard Beliveau, which seemed to have more details and specifics. I found it to be easy to read and understand, beautifully illustrated, and quite helpful. One thing I do believe now, my typical diet was a slow, steady activation of the dormant cancer triggers that exist in every human being. And changing it radically will stop pressing the trigger, and may in turn activate some defense mechanisms. As always, I shall keep you posted. Remember, it all starts like the photo at the left, and it ends like the photo at the right. But BOTH of them can get cancer. I now view sugar as a poison, and it certainly affects the level of my willpower. Saying "No" is very easy, and it gets easier day by day!
guidelines, but sparse on specifics - like just how much of food X should be eaten per day or week. I went ahead and ordered it anyway. And I also ordered a second book, Foods to Fight Cancer: Essential Foods to Help Prevent Cancer, by Richard Beliveau, which seemed to have more details and specifics. I found it to be easy to read and understand, beautifully illustrated, and quite helpful. One thing I do believe now, my typical diet was a slow, steady activation of the dormant cancer triggers that exist in every human being. And changing it radically will stop pressing the trigger, and may in turn activate some defense mechanisms. As always, I shall keep you posted. Remember, it all starts like the photo at the left, and it ends like the photo at the right. But BOTH of them can get cancer. I now view sugar as a poison, and it certainly affects the level of my willpower. Saying "No" is very easy, and it gets easier day by day!
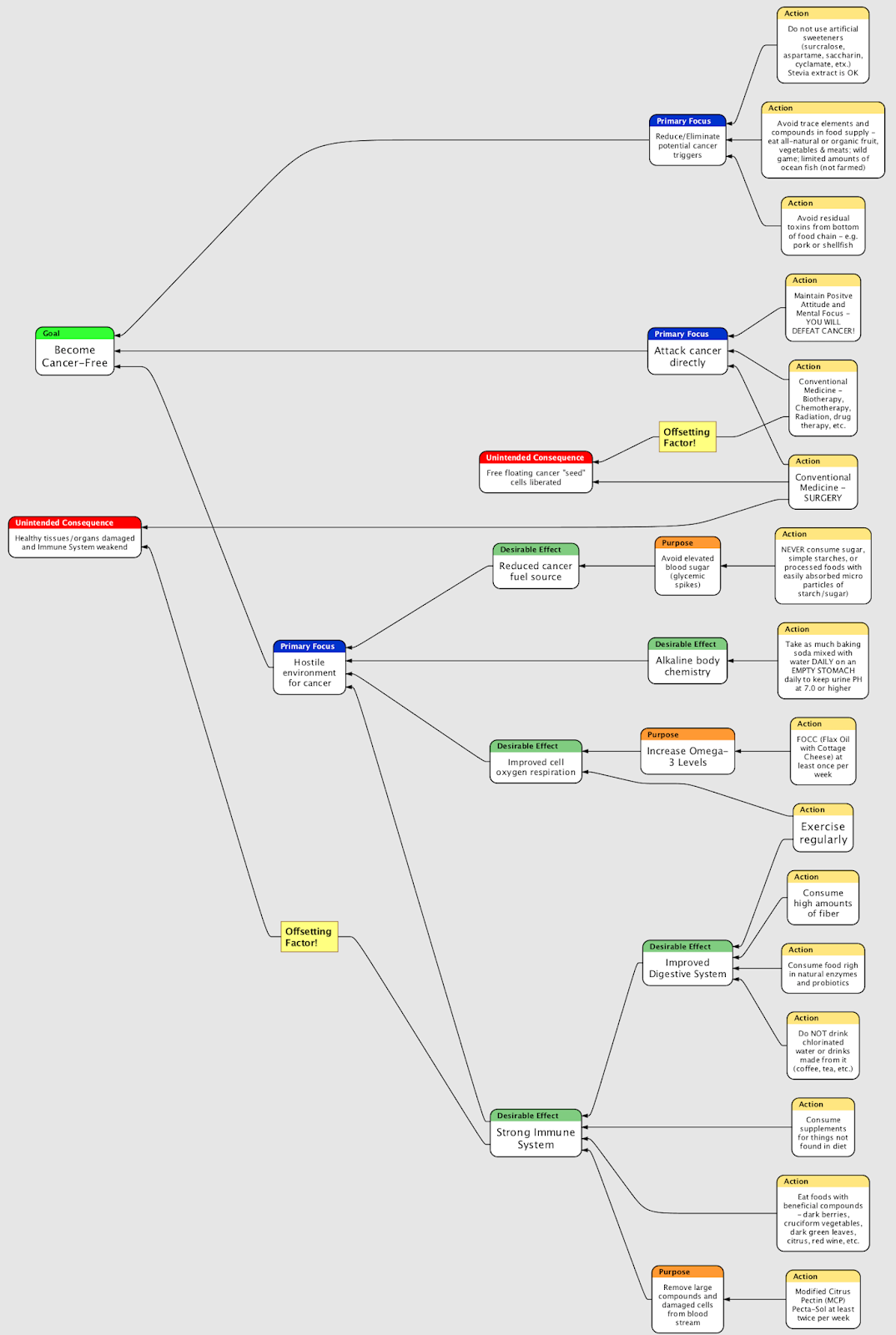
Sure, all of us in the US have heard over and over again, ad nausem, "Diet and exercise! Diet and exercise! Diet and exercise! Diet and exercise!..." And all of us find it easier to eat what we like and do as we please (like chowing down on ice cream from the carton with a big spoon in front of the TV). There's no short term effects of poor diet and inactivity, and the long term effects create a feedback loop - the worse your diet and less you exercise, the easier it is to eat junk and do nothing. Taking myself as an example, there are few folks that pursued bad food and inactivity with the religious fervor that I did. It would take something really big to change my mind about this "I'll die fat but happy" attitude - say a deadly disease or something! Yet encouragement from Crystal, my RN health advisor, and Dr. Lamm, and others has helped fill in the details of what to change. What we are doing now is eating only things that were described in the Bible as "clean" and avoiding things described as "unclean." Though I am a Christian, I did not adopt this plan out of religious reasons. And we are certainly not keeping Kosher! In addition to that, we are avoiding sucrose (table sugar), HFCS high fructose corn syrup (super-sugar), and all artificial sweeteners including aspartame, saccharine, Splenda, xylitol, sorbitol, and other "-ol" sugars. The book suggests that, as far as your blood glucose is concerned, HFCS compares to table sugar like opium compares to poppies! Very nasty stuff indeed, and pervasive in the US food supply...
The list of things to avoid is pretty short and simple from a practical basis:
NO Sugar, High Fructose Corn Syrup, or artificial sweeteners
NO Pork
NO Shellfish
NO Processed flour (of any kind)
NO Processed foods (like hot dogs, cheese whiz, or ketchup)
NO Deep-Fat-Fried foods (chips, fries, corn dogs, etc.)
NO Chlorinated water
What's left? Sweeten with stevia (leaf extract), honey, real maple syrup (all in moderation) or nothing at all. Get organic or "natural" (no hormones, antibiotics, vegetarian diet) beef and poultry, organic vegetables (less important if the peel is not eaten, like citrus) and herbs, fish with fins and scales (no catfish, shark, eels). Whole grains, soaked or sprouted to activate enzymes and healthful bacteria. Lots and lots of fiber. Limit meats. Eat more fish. Avoiding chlorine avoids killing healthful bacteria and crippling natural enzymes in the digestive tract. There is a sound, scientific basis to avoid "unclean" foods. Pigs and shellfish are at the bottoms of their respective food chains, and while their systems clean most pollutants effectively away, the trace amounts are respectively higher than in other foods that are higher in the chain. So avoid them. Even some fish that have fins and scales are also bottom feeders (like tilapia) and should also be avoided. It was a big pain to figure out, but the food that we eat now per the rules above is delicious! Will it work? I think there's sufficient evidence to indicate it will help a lot, but 45+ years of bad eating habits cannot be overcome in a month or two. And it is a far more pleasant way to address the digestive tract than colonics, working from the input rather than the output side!
I think there's sufficient evidence to indicate it will help a lot, but 45+ years of bad eating habits cannot be overcome in a month or two. And it is a far more pleasant way to address the digestive tract than colonics, working from the input rather than the output side!
In a completely unrelated topics, I won't be updating the blog for the next 8-10 days while we are in Acapulco. Also, there was some unusual seismic activity in Northern Utah last evening. Experts are still baffled as to the source. Some mysteries may never be solved...
 Why do I write this blog about bladder cancer? Besides the fact that it helps me to organize my thoughts and data, provides an avenue for catharsis, and feeds my questionable need to be the center of attention, it also fills an information gap. If you read much about bladder cancer on the internet, you find frequently that it is the 4th most common cancer among men. So you would think that there is a lot of information shared out in the cyberspace about it. I dinked around the internet for several weeks looking for others in the same situation. The Bladder Cancer Web Cafe is a great store of information, and there are a lot of stories to read there. Many (if not most) of them are sad stories. And the information is clinical, unvarnished, and very hard to internalize - especially after the shock of diagnosis. Learning too much about what MIGHT happen is potentially nauseating business, and such detailed knowledge makes it very hard to focus on a positive outcome. Add to all this that the specific, practical details of how to deal with TURBT surgery and BCG immunotherapy are left to the imagination. I do not wish to impugn the BC Web Cafe. It's just that it was not what I needed early in the process. Now that I have internalized my condition and have dealt with it on both emotional and intellectual bases, I find the Web Cafe to be a highly useful information source. I even list it prominently in my link list found halfway down the column to the left. But it is far from the first place I would send folks.
Why do I write this blog about bladder cancer? Besides the fact that it helps me to organize my thoughts and data, provides an avenue for catharsis, and feeds my questionable need to be the center of attention, it also fills an information gap. If you read much about bladder cancer on the internet, you find frequently that it is the 4th most common cancer among men. So you would think that there is a lot of information shared out in the cyberspace about it. I dinked around the internet for several weeks looking for others in the same situation. The Bladder Cancer Web Cafe is a great store of information, and there are a lot of stories to read there. Many (if not most) of them are sad stories. And the information is clinical, unvarnished, and very hard to internalize - especially after the shock of diagnosis. Learning too much about what MIGHT happen is potentially nauseating business, and such detailed knowledge makes it very hard to focus on a positive outcome. Add to all this that the specific, practical details of how to deal with TURBT surgery and BCG immunotherapy are left to the imagination. I do not wish to impugn the BC Web Cafe. It's just that it was not what I needed early in the process. Now that I have internalized my condition and have dealt with it on both emotional and intellectual bases, I find the Web Cafe to be a highly useful information source. I even list it prominently in my link list found halfway down the column to the left. But it is far from the first place I would send folks.
In addition the Web Cafe's personal experiences and blogs are unattractively displayed, poorly organized, and highly variable in information content - plus they are full of gaps regarding practical details. I am not complaining, because the price is certainly right - absolutely free! I read some on Cancer Compass, but half the topics there are about bladder cancer in pets - a serious topic, but hardly in the same league as human disease.  If you are politically minded, the Bladder Cancer Advocacy Network site is well organized and full of good basic information. The BCAN focuses on informing the public at large about Bladder Cancer, and advocating more research into it. The sad truth is that bladder cancer is a "boring" subject - not sexy enough for most aspiring doctors and researchers to specialize and pursue new research, and not well-known enough for most funding sources to care about. Sadly BCAN's founder passed away on June 29, 2008 after an eight year battle. His wife and friends continue to run the site and maintain the advocacy. Other sites (also included in my link list found halfway down the column to the left) from the American Cancer Society and National Cancer Institute provide summary information about many topics, but nothing very practical for day to day living.
If you are politically minded, the Bladder Cancer Advocacy Network site is well organized and full of good basic information. The BCAN focuses on informing the public at large about Bladder Cancer, and advocating more research into it. The sad truth is that bladder cancer is a "boring" subject - not sexy enough for most aspiring doctors and researchers to specialize and pursue new research, and not well-known enough for most funding sources to care about. Sadly BCAN's founder passed away on June 29, 2008 after an eight year battle. His wife and friends continue to run the site and maintain the advocacy. Other sites (also included in my link list found halfway down the column to the left) from the American Cancer Society and National Cancer Institute provide summary information about many topics, but nothing very practical for day to day living.
So I looked for individual blogs regarding Bladder Cancer, and I found only two that were specific and hopeful. One is written by a fellow from Canada who spends his summers in Florida. He had the radical surgery (which I still hope to avoid) and is enjoying life and feeding his travel habit. He has only been blogging since December, 2007, though his struggle has been ongoing since July of 2000. He believes his cancer is in full remission, and there is a lot of interesting stuff on his blog, intermixed with advertisements and other items that are not to my taste.
Another blog that my brother found right away is written by David Ferdinando, a fellow in Kent (near London) who posts under the name "A Dived Ref," which is a partial anagram of his name and an obscure reference to football (soccer in the US). His age is close to mine, and he is about two years into his battle - 19 months ahead of me. The British treatment protocol is slightly different from the American one for BCG, so he is now nearing the completion of his BCG treatments - the last one being scheduled for this upcoming Monday. The BCG is working for him, and he looks forward to a normal life and life-span in the future. He's even embarking on a new college-level series of courses to study history, a passion of his. So he's planning on being around a while longer! David's blog is arranged like a normal blog diary, so you will have to read most of it to get to know him and his situation. It's brutally honest and so it's a great way to understand the emotional ups and downs of a bladder cancer patient and a guy nearing the age of 50. It does take some time to get through, however.
So I found myself surfing all over the internet like a dog looking for a virtual bone. To borrow from Bono and U2,  "I have climbed highest mountain, I have run through the fields, Only to be with you, Only to be with you. I have run, I have crawled, I have scaled these city walls, These city walls, Only to be with you. But I still haven't found what I'm looking for..." You may wonder what it is that I'm looking for. It's simple, really. I'm looking for stories of men around my age who have had bladder cancer of my grade and stage and survived it for 10-30 years WITHOUT radical surgery. Stories about the ins and outs of the American medical treatment system, with details on evaluating the options objectively, listing the choices that best guarantee a positive outcome. Stories with real details about what one goes through and what one must actually do to prepare mentally and spiritually. Stories with practical, helpful, and useful information about what to do (and NOT do), where to go, what to buy, what to avoid, and what to expect. Stories that do not rely on standard medical advice in a vacuum. Stories that do not lean solely on self, doctors, systems, proven treatments, or some "mysterious healing force" for all their hope, but also recognize that God is real, He is in charge, and that He arranges everything for MY ultimate good. Stories that are well organized, easy to read and understand. And stories all told with compassion, accuracy, and humor.
"I have climbed highest mountain, I have run through the fields, Only to be with you, Only to be with you. I have run, I have crawled, I have scaled these city walls, These city walls, Only to be with you. But I still haven't found what I'm looking for..." You may wonder what it is that I'm looking for. It's simple, really. I'm looking for stories of men around my age who have had bladder cancer of my grade and stage and survived it for 10-30 years WITHOUT radical surgery. Stories about the ins and outs of the American medical treatment system, with details on evaluating the options objectively, listing the choices that best guarantee a positive outcome. Stories with real details about what one goes through and what one must actually do to prepare mentally and spiritually. Stories with practical, helpful, and useful information about what to do (and NOT do), where to go, what to buy, what to avoid, and what to expect. Stories that do not rely on standard medical advice in a vacuum. Stories that do not lean solely on self, doctors, systems, proven treatments, or some "mysterious healing force" for all their hope, but also recognize that God is real, He is in charge, and that He arranges everything for MY ultimate good. Stories that are well organized, easy to read and understand. And stories all told with compassion, accuracy, and humor.
One would hope that between all the porn sites, advertisements, gaming sites, wikipedias, propaganda, general bullshit, and information overload that permeates cyberspace that there would be dozens of stories as I have described above. Such is not the case. I believe there are three reasons for their absence. First, the internet is still pretty new, so 10, 20, 30 years ago when folks might have survived this cancer there was no blog vehicle to record it. Second, there have been improvements in medicine, surgical techniques, BCG maintenance schedules, and the like that have only been implemented in the last 3-10 years, so increased survival episodes have yet to play out and work their way into the bladder cancer statistics. And third, success stories are much less interesting than tragedies, and so authors of such stories are much less motivated to share them. So dear reader, if you have suffered through to the end of this post, you are pretty much stuck with my blog in my little corner of cyberspace for the time being. Hopefully others will follow, and everyone will benefit. Until then, be advised that all statements in this blog (unless otherwise attributed) are my own thoughts, and as such they are worth no more than you paid for them! Now back to some more U2:
I believe in the kingdom come
Then all the colors will bleed into one
Bleed into one
Well yes I'm still running
You broke the bonds and you
Loosed the chains
Carried the cross
Of my shame
Of my shame
You know I believe it
I was quite surprised to get a call from Dr. Donald L. Lamm in the early afternoon on Labor Day, Monday, September 1. He told me that he was using the day to catch up on things, and he apologized for taking so long to get back to me. I asked him if he had read all the information I had sent to him, and he surprised me a little by responding in the affirmative. I had downgraded my expectations somewhat after my consult with Dr. X, although I had some hopes that Dr. Lamm would have some new inputs on BCG maintenance treatments scheduled to begin a week after my cystoscope on October 23 - IF all goes well. Certainly Dr. X thought highly of Dr. Lamm in the BCG arena. My wife and I were both home, and Dr. Lamm endorsed my plan of putting him on speaker phone so that we had hands free for note taking and that we both could listen. Dr. Lamm's resume is quite impressive, he has written a number of textbooks, and he has the advantage of years of experience over both Dr. Hopkins and Dr. X.
I had downgraded my expectations somewhat after my consult with Dr. X, although I had some hopes that Dr. Lamm would have some new inputs on BCG maintenance treatments scheduled to begin a week after my cystoscope on October 23 - IF all goes well. Certainly Dr. X thought highly of Dr. Lamm in the BCG arena. My wife and I were both home, and Dr. Lamm endorsed my plan of putting him on speaker phone so that we had hands free for note taking and that we both could listen. Dr. Lamm's resume is quite impressive, he has written a number of textbooks, and he has the advantage of years of experience over both Dr. Hopkins and Dr. X.
We grabbed notepads and pens quickly and proceeded. My $300 fee included his review of my records and a "10 minute phone consultation," so I wanted to get as many questions answered as we could in the allotted time. I asked if he had any introductory remarks, and he told me he had written a brief report which he could forward to me via email. We exchanged email addresses for that purpose. He generally supported the original diagnosis, but was a bit more specific on the language - "You have high grade T1 bladder cancer with high grade Ta recurrent TCC on repeat resection, and you appropriately elected a trial of 6 BCG immunotherapy treatments." Dr. Lamm added that he had a detailed summary written, and suggested we proceed with questions.
 Were any additional risks added from the bladder perforation during my first TURBT?
Were any additional risks added from the bladder perforation during my first TURBT?
No. Well, not absolutely no. According to the surgical report this perforation was minor and well investigated, so the chances of any problems are very small.Would any additional diagnostics be useful?
CT Urograms on the upper tract, which would be a routine part of your follow-up care anyway.The radiology report from my CT scan indicated inflammation possible outside the bladder and/or in the transverse colon. Is there any cause for concern?
Not specifically. Dietary changes should address the diverticula. I'd advise you to consult your family doctor about this. (Still a question for Dr. Chuck!)
I live at about a mile elevation. Is that a concern? Should I consider supplemental oxygen?
No. Doing some routine exercise would alleviate any issues of that nature.What is your opinion on complementary Oncovite vitamin therapy?
A good diet will be more powerful than any vitamin regimen, including Oncovite. I just bought a six months supply of Oncovite. Should I discontinue?
I just bought a six months supply of Oncovite. Should I discontinue?
No - by all means take them. They won't do any harm, but you don't need them.What about Modified Citrus Pectin?
The data on MCP are not as strong as the data for Oncovite, so again a good diet will be more beneficial. MCP should not hurt anything, but it probably won't help.
And hyperthermia?
We always use localized hyperthermia in conjunction with low dose chemotherapy. This regimen is used sometimes when BCG fails.Hyperbaric, or others?
Look, you don't need any of that. The best hope to combat the disease is to follow my recommended courses of BCG maintenance, which I outlined on the written recommendation. These things like hyperbaric and hyperthermia are to fight cancer. You don't have any cancer right now, so the BCG is the thing that will best combat recurrence and progression. At this point those other things would be a waste of time and money.What about specific dietary restrictions, such as avoiding sugar, or a radical change?
The diet you described on your medical history form is not too bad. I think there are a few changes that you could make to do better. I imagine you may have already implemented some changes?Yes, I would describe it as a radical change - no pork or shellfish, no sugar, no processed food, no processed flour, no fried food, and organic or natural on everything else.
Well that's pretty close to what I'd recommend. You need to make sure that you are getting a minimum of 10 servings of fruit or vegetables daily.We're in the early restrictive phase of the diet, but we will be up to that by next week.
Excellent. I will send along a report on foods and supplements that you might want to consider in addition. And if you keep up this type of diet, I expect your gout will clear up on its own. Limit red meat to once per week. Here's your order of focus:
1) The most important thing to do is the BCG maintenance as I've recommended in your report
2) The next single biggest contributor to keeping cancer-free is a permanent dietary change along the lines you are doing now. A vegetarian diet is optimal for reduction of carcinogens, so limit animal protein.
3) The next most critical thing is to do some form - any form - of regular exercise. Jogging, swimming, biking, whatever. It has to be more than walking around your office building.I was afraid you'd say that last one!
{Laughs}If no cancer is observed on October 23, do the BCG?
Yes.Do you recommend any other diagnostics?
FISH urine test. Do it at six months. You had a positive FISH before, and a positive FISH at 3 months may be false. BCG needs six months to work, at which point you need a negative FISH result.
If cancer is observed on the October 23 cystoscope, is radical cystectomy is indicated?
If it's something less than high grade T1, you cannot conclude that BCG has failed. It takes six full months to do its work.Can that grading and staging be determined via cystoscope?
No. You always have to resect to see what it is. (This appears to be a significant difference of opinion from Dr. Hopkins and Dr. X)
For high grade or progression, radical surgery is indicated?
Yes, remove the bladder and 10-15% of the lymph nodes. For urinary diversion I recommend the orthotopic neobladder. I think you'll be happier with that. (Dr. Lamm did not mention prostate, but I infer that it is also removed)
How long would I have to arrange for it and get it done?
Three months maximum.I understand there are significant risks for loss of sexual function, incontinence, or no-continence associated with radical surgery.
Not significant if it's done properly.Any pouch or neobladder techniques better than others?
I recommend an orthotopic ileal neobladder. It will preserve a normal lifestyle for you.Any surgeons you would recommend for the radical cystectomy?
Well, there's a fellow in Phoenix, Arizona that I like a lot. His name is Lamm. {Laughs}I thought you had retired from the surgery business?
Not at all. I did one last week. I do two to three every month.If BCG maintenance continues, how long before we go back to TURBT and restart everything?
It depends on the grade. I might advise chemo plus hyperthermia. And I would never want you to reinduct with six BCG treatments. We would likely go on extended maintenance BCG, reducing dosages based on your reaction symptoms.
We thanked Dr. Lamm and concluded the call. In short order I received his written second opinion, which was a full page summarizing my history and a half page of specific recommendations. I also received his dietary advice in a separate file. The recommendation portion of his report appears below:
Impression and recommendations:
1. High grade, T1 bladder cancer with high grade Ta recurrent TCC on repeat resection. He is now post 6 week induction BCG, which was tolerated with moderate symptoms. He had Mitomycin C after the repeat resection, and not after the first due to bladder perforation. He has been offered cystectomy with ileal loop diversion and has elected (appropriately in my opinion) a trial of BCG immunotherapy. At his young age he would appear to be a candidate for an orthotopic ileal neobladder should radical cystectomy be required. I believe he would be happier with that diversion. Extended lymphadenectomy should, in my opinion, also be done if cystectomy is required. I would strongly recommend that he receive 3 week maintenance BCG. With his symptoms during the first course I would recommend reducing the dose to 1/3 and giving up to 3 instillations at 3, 6, 12, 18 and 24 months, then yearly to 6 years, then at 8, 10 and 12 years to reduce the increased risk of disease progression after 10 years as reported in the Memorial Sloan-Kettering series. He now has an exceptionally good diet. Neither Oncovite nor Intron A significantly improves disease free status when the above maintenance schedule is used, but should be considered if he fails or does not receive the optimal schedule as described above. While CIS has not been seen, with high grade/recurrent disease it may be present, and he is certainly at long term risk for recurrence, progression and extravesical disease in the prostate and upper tracks. Periodic CT urogram and biopsy of the prostatic urethra and upper tract cytology may reduce that risk. I would recommend repeating his FISH at 6 months, and would follow him with cystoscopy/cytology every 3 months for 2 years, every 6 months for 2 years and then yearly. At his request I will send him a list of dietary and nutritional supplements that some evidence suggests is beneficial in bladder cancer. I also recommend regular physical exercise.
I also recommend regular physical exercise.
Don Lamm, MD
Certainly a better outlook than what I got from Dr. X, and much more helpful on a practical level. It's a bargain at $300. As I had agreed, I forwarded the BCG regimen and a copy of the full Lamm report to Dr. X via email. He replied quickly with a brief "Thanks for the update. Sounds like a reasonable plan." I need to get this Q&A summary, the Q&A summary from Dr. X, Lamm's full report and dietary recommendations, and Dr. X's reply to Dr. Hopkins for his review and consideration. Dr. X had felt that Dr. Hopkins would be willing to adopt Lamm's approach without question. My preference would be that Hopkins and Lamm would collaborate on my case. I'd certainly be willing to pay for it. Stay tuned...
I traveled from Utah to Indianapolis last Thursday-Sunday, and I stayed with Lee, a good friend from college (like Dr. Chuck). We saw the original cast of Beatlemania in their Magical Mystery Tour concert, we did some hiking in the woods, and we managed to take in a AAA ball game where the Indianapolis Indians spanked the Louisville Bats handily. I also had an appointment with a urological oncologist who had been described by my doctor as "brilliant" and whose credentials had been approved by Dr. Chuck. Naturally my expectations were high, and probably unrealistic. I had hope that he would confirm that the diagnosis was either correct or perhaps even less severe.  I expected he would be familiar with cutting edge treatments in the field - perhaps some that Dr. Hopkins was unaware of. I wanted him to tell me if additional risk was created from the bladder puncture in the first surgery, and what could/should be done about that. I wanted to quiz him about best-case and worst-case scenarios, and I thought he might have information on more than the two options I had heard to date (BCG best case, radical cystectomy worst case).
I expected he would be familiar with cutting edge treatments in the field - perhaps some that Dr. Hopkins was unaware of. I wanted him to tell me if additional risk was created from the bladder puncture in the first surgery, and what could/should be done about that. I wanted to quiz him about best-case and worst-case scenarios, and I thought he might have information on more than the two options I had heard to date (BCG best case, radical cystectomy worst case).
The problem with high expectations is that your probability of being disappointed is also high. And so it was with my second opinion. While the doctor was as helpful as he could be, and he took longer than he planned to answer all my questions thoroughly, most of my hopes and expectations were not realized. He had not reviewed my records in detail. He did not personally verify the diagnosis. And most of all, he made it clear that he only supported courses of actions that had been thoroughly tested in controlled environments with sufficient test subjects that were published in peer-reviewed journals. While this is both safe and prudent for him, it limited the information he provided to things that would have been easy for me to research on my own. While I did learn some new and valuable information, it was not worthy of my time investment. So I do not recommend him specifically, and I will refer to him as Dr. X. There's no issue with Dr. X - he is certainly representative of mainstream medical opinion. And therefore there is no reason for you to seek him out rather than a competent physician in your local area. The following is a summary of my consultation with Dr. X on Friday, August 29, which lasted for more than an hour.
Dr. X made a great effort to distinguish between cancer RECURRENCE and cancer PROGRESSION. The most important factor in determining whether to continue with BCG treatments and simple TUR surgeries is whether or  not the cancer PROGRESSES. If you have read any of my other posts, you know that my cancer has been classified as T1 and Grade 3 (T1-G3). The T score is known as "staging" and it measures PROGRESSION. Grade is the strength/differentiation score. A great summary of bladder cancer basics may be found HERE. Like in golf, low numbers are better than high numbers. So if you have bladder cancer, T1-G1 is a nuisance to deal with for lifetime, but it is very unlikely to progress. If you have anything more, progression (e.g. going from T1 to T2, T3, etc.) is a guessing game. Grade and recurrence are the only tools widely used to judge probability of progression. My G3 is the max bad score you can have, and my chance of PROGRESSION is already high. If RECURRENCE happens quickly, the indicators that the cancer will PROGRESS are maxed out, and the standard treatment is radical cystectomy. Dr. X. flatly stated that radical cystectomy has the single, highest survivability statistics over any other standard treatment. It also has a lot of risk and lifestyle impacts, so most patients (myself included) want very much to avoid it. Next we went into my list of questions.
not the cancer PROGRESSES. If you have read any of my other posts, you know that my cancer has been classified as T1 and Grade 3 (T1-G3). The T score is known as "staging" and it measures PROGRESSION. Grade is the strength/differentiation score. A great summary of bladder cancer basics may be found HERE. Like in golf, low numbers are better than high numbers. So if you have bladder cancer, T1-G1 is a nuisance to deal with for lifetime, but it is very unlikely to progress. If you have anything more, progression (e.g. going from T1 to T2, T3, etc.) is a guessing game. Grade and recurrence are the only tools widely used to judge probability of progression. My G3 is the max bad score you can have, and my chance of PROGRESSION is already high. If RECURRENCE happens quickly, the indicators that the cancer will PROGRESS are maxed out, and the standard treatment is radical cystectomy. Dr. X. flatly stated that radical cystectomy has the single, highest survivability statistics over any other standard treatment. It also has a lot of risk and lifestyle impacts, so most patients (myself included) want very much to avoid it. Next we went into my list of questions.
Do you concur with the grading and staging of my cancer?
Yes.Did you look at the reports, slide images, or both?
My staff usually looks at the most detailed data they can get. I'm not sure if they were able to get the slide images for you or not.
Do you concur with the diagnosis and recommended course of treatment?
Yes.Were any additional risks added from the bladder perforation during my first TURBT?
Theoretically there is a small risk, but nothing has ever been proved to propagate from a perforation. So I don't believe there is any real additional risk.Would any additional diagnostics be useful?
The only thing you can do is another CT scan.That would only work after something got big enough to be a problem, correct?
Correct.What about an exploratory surgery?
You could not see anything that way until it got big enough to see visually, so it's no better than the CT scan. And nobody would do it.The radiology report from my CT scan indicated inflammation possible outside the bladder and/or in the transverse colon. Is there a probability or risk of abdominal or lymphatic cancer already in progress?
You would have to ask a gastrointestinal doctor for specifics, but I find it doubtful.How would it be diagnosed?
Via colonoscopy.I'm scheduled to get my first one of those next summer after I turn 50. Do you believe the report suggests I should get one sooner?
No, that should not be necessary. Again, you could ask a GI doctor. (Looks like a question for Dr. Chuck)
I have heard that cancer does not like oxygen. My house is at about a mile elevation. Is that a concern? Should I consider supplemental oxygen?
No. Not at all.Do you have an opinion on complementary therapies in addition to the BCG, such as vitamins, MCP, hyperthermia, hyperbaric, or others?
Nothing has been proven to my satisfaction to be helpful. Of course, any of these things COULD help, along with Taxol or other stuff from the Amazon rain forest. There would be an underlying chemical basis, and that would need to be studied and tested under controlled conditions. Just make sure that anything you try won't hurt you, and it's possible that some of it might help.What about specific dietary restrictions, such as avoiding sugar, or a radical change?
Won't matter. You already have cancer and nothing in diet can change that. Diet MIGHT help someone avoid getting cancer, but once you've got it, you've got it. (NOTE: I do not agree with Dr. X on this subject)So there's really NOTHING I can do in addition to the BCG to improve my odds?
I doubt it. I think you're doing everything you can. Just make sure you don't try anything that might hurt.Did you read the information about Oncovite or MCP in my materials?
No.What are my odds at this point?
We have to segregate your RECURRENCE odds from your PROGRESSION odds. Your odds of PROGRESSION are 50%. Your odds of recurrence are significantly higher than that. Early recurrence for your grade (G3) is a strong indicator for progression. How long before the recurrence is not considered "early" and we can go back to TURBT to remove it?
How long before the recurrence is not considered "early" and we can go back to TURBT to remove it?
I'd say a year to two years. I really like that one-year threshold, myself. I'd go back to TUR for a patient who had no recurrence for a year, unless there's evidence of progression.Can't progression only be evaluated through resection and lab work?
Often you can tell with the cystoscope.Do you recommend any other diagnostics?
Urine cytology also.I'm also doing a consultation with Dr. Lamm. Are you familiar with him and his work?
Yes, very much so. He and Dr.(I missed the name) pioneered BCG treatments, and his paper in the late 90s documented the effectiveness of maintenance therapy.
Do you have a recommended BCG regimen?
I generally do six doses, and occasionally do maintenance.
Why don't you always do maintenance, if the paper documented the effectiveness?
Because only six patients were able to tolerate the maintenance treatments to their conclusion, I think two or three years. So while the initial sample was big, the end sample was small.
Dr. Lamm has done some recent work with reduced dosages and increased frequency to improve tolerance by patients. Do you have any opinions about that?
If you are doing a consult with Dr. Lamm, you should follow his recommendations for your specific case to the letter. He knows more about it than either Dr. Hopkins or myself. I'd like to know what he recommends for my own education. (I agreed to email him the summary.)
If radical cystectomy is indicated after my October 23 cystoscope, how long do I have to arrange for it and get it done?
If progression is observed, I'd do it immediately. I'd like you on the operating table within six weeks. If not, maybe two to three months. Say 90 days maximum.
If radical cystectomy is indicated, does that always mean taking multiple organs out like prostate, lymph nodes, etc.?
Yes. The cystectomy is really a misnomer. We will take out your bladder, your prostate, and several lymph nodes.What about not taking the "yard sale" approach?
It's not safe. Nobody in the US would perform such a surgery. You should really not focus on this outcome. A positive attitude is going to be very helpful for your upcoming treatments.I agree. But with potentially only six weeks to get it done in the worst case, that would not leave much time to get educated, choose a physician, get the workups, etc.
That's a good point.I read that there's a 2% chance of dying on the table.
It used to be 3% but it's down to 1% now that you won't leave the hospital.I have read that 30% of prostatectomy patients die within 5 years.
That's not accurate at all. I don't know the number, but it's small, like 2-3%.I have also read that 90% of prostatectomy patients lose their "recreational facilities" forever.
Count on it. And count on a 5-10% chance of daytime incontinence and a 15-20% chance of nighttime incontinence. On the other end of the scale there's a 20% chance of needing to do self-catheterizations.What about "nerve sparing" techniques?
Maybe there are some small improvements in this field. I'm not familiar.Any pouch or neobladder techniques better than others?
Most common is the Studer. USC uses T-pouches. I'm not aware of any significant advantages or drawbacks to any one procedure.Any surgeons you would recommend for the radical cycstectomy?
Bernie Bochner at Memorial Sloan-Kettering in Manhattan, Don Skinner at USC in Los Angeles (retired in 2017), or Seth Lerner at Baylor in Houston. I can get you a referral for Bochner if you need it.What's your final summary of my prognosis?
We know certain things that work. BCG works sometimes, but we don't know the exact mechanism. Maintenance therapy works. Removing the prostate and lymph nodes in addition to the bladder works. Radical cystectomy provides the absolute highest chances of survival. Do whatever Lamm recommends for BCG for your specific case. You are doing everything you can (and more) to improve your chances. Keep a positive attitude.Thank you for your time.
Obviously this is a lot to process. My original plan was to stay positive and focus on a positive outcome for October. I had assumed there would be ample time to research the flip side and/or try other therapies if the news is bad. Now I will have to learn more about the bad outcome while staying focused on the positive one. I hope that my session (via phone) with Dr. Lamm is more encouraging.

 .
.
 My friend Kathie wrote a comment on the Dr. Lamm post and referred to a book by another doctor (David Servan-Schreiber) that supports the diet/exercise regimen for battling cancer. Anti-Cancer: A New Way of Life describes some lifestyle changes that can be effective in keeping cancer in remission. I looked at the link and read some previews from the book both there and on Amazon. After only a few months of research on the general topic of cancer and the specific topic of bladder cancer, I have found that there are five options frequently found when searching the internet (or other areas) for adjunct or alternative therapies for cancer treatment.
My friend Kathie wrote a comment on the Dr. Lamm post and referred to a book by another doctor (David Servan-Schreiber) that supports the diet/exercise regimen for battling cancer. Anti-Cancer: A New Way of Life describes some lifestyle changes that can be effective in keeping cancer in remission. I looked at the link and read some previews from the book both there and on Amazon. After only a few months of research on the general topic of cancer and the specific topic of bladder cancer, I have found that there are five options frequently found when searching the internet (or other areas) for adjunct or alternative therapies for cancer treatment. The Amazon review links indicate that it's good for self-attitude and general food
The Amazon review links indicate that it's good for self-attitude and general food  guidelines, but sparse on specifics - like just how much of food X should be eaten per day or week. I went ahead and ordered it anyway. And I also ordered a second book, Foods to Fight Cancer: Essential Foods to Help Prevent Cancer, by Richard Beliveau, which seemed to have more details and specifics. I found it to be easy to read and understand, beautifully illustrated, and quite helpful. One thing I do believe now, my typical diet was a slow, steady activation of the dormant cancer triggers that exist in every human being. And changing it radically will stop pressing the trigger, and may in turn activate some defense mechanisms. As always, I shall keep you posted. Remember, it all starts like the photo at the left, and it ends like the photo at the right. But BOTH of them can get cancer. I now view sugar as a poison, and it certainly affects the level of my willpower. Saying "No" is very easy, and it gets easier day by day!
guidelines, but sparse on specifics - like just how much of food X should be eaten per day or week. I went ahead and ordered it anyway. And I also ordered a second book, Foods to Fight Cancer: Essential Foods to Help Prevent Cancer, by Richard Beliveau, which seemed to have more details and specifics. I found it to be easy to read and understand, beautifully illustrated, and quite helpful. One thing I do believe now, my typical diet was a slow, steady activation of the dormant cancer triggers that exist in every human being. And changing it radically will stop pressing the trigger, and may in turn activate some defense mechanisms. As always, I shall keep you posted. Remember, it all starts like the photo at the left, and it ends like the photo at the right. But BOTH of them can get cancer. I now view sugar as a poison, and it certainly affects the level of my willpower. Saying "No" is very easy, and it gets easier day by day! I think there's sufficient evidence to indicate it will help a lot, but 45+ years of bad eating habits cannot be overcome in a month or two. And it is a far more pleasant way to address the digestive tract than colonics, working from the input rather than the output side!
I think there's sufficient evidence to indicate it will help a lot, but 45+ years of bad eating habits cannot be overcome in a month or two. And it is a far more pleasant way to address the digestive tract than colonics, working from the input rather than the output side! Why do I write this blog about bladder cancer? Besides the fact that it helps me to organize my thoughts and data, provides an avenue for catharsis, and feeds my questionable need to be the center of attention, it also fills an information gap. If you read much about bladder cancer on the internet, you find frequently that it is the 4th most common cancer among men. So you would think that there is a lot of information shared out in the cyberspace about it. I dinked around the internet for several weeks looking for others in the same situation. The Bladder Cancer Web Cafe is a great store of information, and there are a lot of stories to read there. Many (if not most) of them are sad stories. And the information is clinical, unvarnished, and very hard to internalize - especially after the shock of diagnosis. Learning too much about what MIGHT happen is potentially nauseating business, and such detailed knowledge makes it very hard to focus on a positive outcome. Add to all this that the specific, practical details of how to deal with TURBT surgery and BCG immunotherapy are left to the imagination. I do not wish to impugn the BC Web Cafe. It's just that it was not what I needed early in the process. Now that I have internalized my condition and have dealt with it on both emotional and intellectual bases, I find the Web Cafe to be a highly useful information source. I even list it prominently in my link list found halfway down the column to the left. But it is far from the first place I would send folks.
Why do I write this blog about bladder cancer? Besides the fact that it helps me to organize my thoughts and data, provides an avenue for catharsis, and feeds my questionable need to be the center of attention, it also fills an information gap. If you read much about bladder cancer on the internet, you find frequently that it is the 4th most common cancer among men. So you would think that there is a lot of information shared out in the cyberspace about it. I dinked around the internet for several weeks looking for others in the same situation. The Bladder Cancer Web Cafe is a great store of information, and there are a lot of stories to read there. Many (if not most) of them are sad stories. And the information is clinical, unvarnished, and very hard to internalize - especially after the shock of diagnosis. Learning too much about what MIGHT happen is potentially nauseating business, and such detailed knowledge makes it very hard to focus on a positive outcome. Add to all this that the specific, practical details of how to deal with TURBT surgery and BCG immunotherapy are left to the imagination. I do not wish to impugn the BC Web Cafe. It's just that it was not what I needed early in the process. Now that I have internalized my condition and have dealt with it on both emotional and intellectual bases, I find the Web Cafe to be a highly useful information source. I even list it prominently in my link list found halfway down the column to the left. But it is far from the first place I would send folks. If you are politically minded, the Bladder Cancer Advocacy Network site is well organized and full of good basic information. The BCAN focuses on informing the public at large about Bladder Cancer, and advocating more research into it. The sad truth is that bladder cancer is a "boring" subject - not sexy enough for most aspiring doctors and researchers to specialize and pursue new research, and not well-known enough for most funding sources to care about. Sadly BCAN's founder passed away on June 29, 2008 after an eight year battle. His wife and friends continue to run the site and maintain the advocacy. Other sites (also included in my link list found halfway down the column to the left) from the American Cancer Society and National Cancer Institute provide summary information about many topics, but nothing very practical for day to day living.
If you are politically minded, the Bladder Cancer Advocacy Network site is well organized and full of good basic information. The BCAN focuses on informing the public at large about Bladder Cancer, and advocating more research into it. The sad truth is that bladder cancer is a "boring" subject - not sexy enough for most aspiring doctors and researchers to specialize and pursue new research, and not well-known enough for most funding sources to care about. Sadly BCAN's founder passed away on June 29, 2008 after an eight year battle. His wife and friends continue to run the site and maintain the advocacy. Other sites (also included in my link list found halfway down the column to the left) from the American Cancer Society and National Cancer Institute provide summary information about many topics, but nothing very practical for day to day living. "I have climbed highest mountain, I have run through the fields, Only to be with you, Only to be with you. I have run, I have crawled, I have scaled these city walls, These city walls, Only to be with you. But I still haven't found what I'm looking for..." You may wonder what it is that I'm looking for. It's simple, really. I'm looking for stories of men around my age who have had bladder cancer of my grade and stage and survived it for 10-30 years WITHOUT radical surgery. Stories about the ins and outs of the American medical treatment system, with details on evaluating the options objectively, listing the choices that best guarantee a positive outcome. Stories with real details about what one goes through and what one must actually do to prepare mentally and spiritually. Stories with practical, helpful, and useful information about what to do (and NOT do), where to go, what to buy, what to avoid, and what to expect. Stories that do not rely on standard medical advice in a vacuum. Stories that do not lean solely on self, doctors, systems, proven treatments, or some "mysterious healing force" for all their hope, but also recognize that God is real, He is in charge, and that He arranges everything for MY ultimate good. Stories that are well organized, easy to read and understand. And stories all told with compassion, accuracy, and humor.
"I have climbed highest mountain, I have run through the fields, Only to be with you, Only to be with you. I have run, I have crawled, I have scaled these city walls, These city walls, Only to be with you. But I still haven't found what I'm looking for..." You may wonder what it is that I'm looking for. It's simple, really. I'm looking for stories of men around my age who have had bladder cancer of my grade and stage and survived it for 10-30 years WITHOUT radical surgery. Stories about the ins and outs of the American medical treatment system, with details on evaluating the options objectively, listing the choices that best guarantee a positive outcome. Stories with real details about what one goes through and what one must actually do to prepare mentally and spiritually. Stories with practical, helpful, and useful information about what to do (and NOT do), where to go, what to buy, what to avoid, and what to expect. Stories that do not rely on standard medical advice in a vacuum. Stories that do not lean solely on self, doctors, systems, proven treatments, or some "mysterious healing force" for all their hope, but also recognize that God is real, He is in charge, and that He arranges everything for MY ultimate good. Stories that are well organized, easy to read and understand. And stories all told with compassion, accuracy, and humor. I had downgraded my expectations somewhat after my consult with Dr. X, although I had some hopes that Dr. Lamm would have some new inputs on BCG maintenance treatments scheduled to begin a week after my cystoscope on October 23 - IF all goes well. Certainly Dr. X thought highly of Dr. Lamm in the BCG arena. My wife and I were both home, and Dr. Lamm endorsed my plan of putting him on speaker phone so that we had hands free for note taking and that we both could listen. Dr. Lamm's resume is quite impressive, he has written a number of textbooks, and he has the advantage of years of experience over both Dr. Hopkins and Dr. X.
I had downgraded my expectations somewhat after my consult with Dr. X, although I had some hopes that Dr. Lamm would have some new inputs on BCG maintenance treatments scheduled to begin a week after my cystoscope on October 23 - IF all goes well. Certainly Dr. X thought highly of Dr. Lamm in the BCG arena. My wife and I were both home, and Dr. Lamm endorsed my plan of putting him on speaker phone so that we had hands free for note taking and that we both could listen. Dr. Lamm's resume is quite impressive, he has written a number of textbooks, and he has the advantage of years of experience over both Dr. Hopkins and Dr. X. Were any additional risks added from the bladder perforation during my first TURBT?
Were any additional risks added from the bladder perforation during my first TURBT? I just bought a six months supply of Oncovite. Should I discontinue?
I just bought a six months supply of Oncovite. Should I discontinue? I expected he would be familiar with cutting edge treatments in the field - perhaps some that Dr. Hopkins was unaware of. I wanted him to tell me if additional risk was created from the bladder puncture in the first surgery, and what could/should be done about that. I wanted to quiz him about best-case and worst-case scenarios, and I thought he might have information on more than the two options I had heard to date (BCG best case, radical cystectomy worst case).
I expected he would be familiar with cutting edge treatments in the field - perhaps some that Dr. Hopkins was unaware of. I wanted him to tell me if additional risk was created from the bladder puncture in the first surgery, and what could/should be done about that. I wanted to quiz him about best-case and worst-case scenarios, and I thought he might have information on more than the two options I had heard to date (BCG best case, radical cystectomy worst case). not the cancer PROGRESSES. If you have read any of my other posts, you know that my cancer has been classified as T1 and Grade 3 (T1-G3). The T score is known as "staging" and it measures PROGRESSION. Grade is the strength/differentiation score. A great summary of bladder cancer basics may be found HERE. Like in golf, low numbers are better than high numbers. So if you have bladder cancer, T1-G1 is a nuisance to deal with for lifetime, but it is very unlikely to progress. If you have anything more, progression (e.g. going from T1 to T2, T3, etc.) is a guessing game. Grade and recurrence are the only tools widely used to judge probability of progression. My G3 is the max bad score you can have, and my chance of PROGRESSION is already high. If RECURRENCE happens quickly, the indicators that the cancer will PROGRESS are maxed out, and the standard treatment is radical cystectomy. Dr. X. flatly stated that radical cystectomy has the single, highest survivability statistics over any other standard treatment. It also has a lot of risk and lifestyle impacts, so most patients (myself included) want very much to avoid it. Next we went into my list of questions.
not the cancer PROGRESSES. If you have read any of my other posts, you know that my cancer has been classified as T1 and Grade 3 (T1-G3). The T score is known as "staging" and it measures PROGRESSION. Grade is the strength/differentiation score. A great summary of bladder cancer basics may be found HERE. Like in golf, low numbers are better than high numbers. So if you have bladder cancer, T1-G1 is a nuisance to deal with for lifetime, but it is very unlikely to progress. If you have anything more, progression (e.g. going from T1 to T2, T3, etc.) is a guessing game. Grade and recurrence are the only tools widely used to judge probability of progression. My G3 is the max bad score you can have, and my chance of PROGRESSION is already high. If RECURRENCE happens quickly, the indicators that the cancer will PROGRESS are maxed out, and the standard treatment is radical cystectomy. Dr. X. flatly stated that radical cystectomy has the single, highest survivability statistics over any other standard treatment. It also has a lot of risk and lifestyle impacts, so most patients (myself included) want very much to avoid it. Next we went into my list of questions.




{kind=link}
{kind=link}
{kind=link}