 I originally wrote this post more than five years ago. In the time since, now more than eleven years cancer-free, I have come to different conclusions and priorities. Even so the message is basically the same.
I originally wrote this post more than five years ago. In the time since, now more than eleven years cancer-free, I have come to different conclusions and priorities. Even so the message is basically the same.There are two things a cancer patient must do to survive:
1) Adopt the correct attitude
2) Adopt the correct "body chemistry"
Nothing else really matters. All the treatments (TURBT, BCG, chemo, radiation, cystectomy or other surgeries, diet, exercise, supplements, etc.) are secondary to these two things. Am I advising you to abandon the "standard of care" and tell your doctors to go to hell? Absolutely not! Attitude and body chemistry can be adjusted completely independent of the treatments you elect to undergo.
It is hard to say which of these two, attitude or chemistry, is more important. The simple fact is this - without the right attitude, a cancer patient will not bother to change their body chemistry. So the sequence is correct:
1) Adopt the correct attitude
2) Adopt the correct "body chemistry"

Step 1 - Let us begin with attitude. How should someone, ANYONE, deal with a cancer diagnosis? Here is the correct attitude:
YOU HAVE TO CHOOSE NOT TO DIE FROM CANCER.
 This is the first line of defense and the bottom line for ANY treatment regimen.
If you choose to accept that your cancer is a death sentence, then ultimately it
will be.
This is the first line of defense and the bottom line for ANY treatment regimen.
If you choose to accept that your cancer is a death sentence, then ultimately it
will be.Don't get me wrong - I am not suggesting willpower for self-healing or other miracle working. This is much more practical. Our culture has conditioned us to accept cancer as a death sentence. Sometimes people survive, and that event is rare enough to be thought of as a miracle, or perhaps a statistical aberration. It is VERY difficult to overcome this conditioning, and the more formal education one has, the more locked-in the conditioning.
People often tell me about cancers, usually a relative or close friend. Since I have cancer, and I have done some things that have been successful to date, they hope against hope that I can offer advice. I generally suggest one or two simple things the cancer patient (not victim) could do in addition to the doctor's recommendations. People rarely pass on the suggestion, and even if they do, the cancer patients almost never try them.
Many otherwise intelligent people abandon reason, almost as if they have operant conditioning, to accept that medical science is the only existing reaction for any recourse against cancer. The hard truth of the matter is that the results for medical success are staggeringly low. Any logical person must therefore realize that the odds are stacked against them. Hopelessness is the default response. And people are not willing to try anything unknown or "unscientific". If this is your situation, you should face the reality of your attitude. By choosing not to try anything extra, you have simply chosen to die.
Here are two examples:
For many years at work I sat beside a brilliant man. It would be reasonable to describe him as a "rocket scientist," or perhaps more accurately a missile engineer. He is also a neighbor who lives 2 blocks away. He was diagnosed with pancreatic cancer that was found to have metastasized. His condition was grave. I went over and shared what I was doing. I even made a small batch of FOCC and showed his wife how easy it was to prepare. She and I both thought it tasted pretty good. He tasted it, made a face, spit it out, and said, "Yech! I will not eat that. It tastes like pancake batter!" I was quite taken aback - standing before him as living proof of success (so far) in battling cancer, a person he knows to be of some intelligence, offering a simple recommendation to follow - yet he chose to ignore my input. It later became clear that he had (at least subconsciously) chosen to die and was not going to be inconvenienced by any extra unpleasantness or hassles suggested by me. Ironically what the doctors are doing to him is far more unpleasant than eating some "pancake batter."

Example two: A friend of my mother's, who was the class valedictorian in her high school and had retired some years ago after a career as a brilliant theoretical physicist, reported that his wife had cancer and it was terminal. I hear this a lot (this was the second one that day), and it really makes me angry. Perhaps cancer will kill you, but to just accept that it will be so seems to me to be fundamentally and morally wrong. This fellow's scenario is typical. His wife has cancer of some type, it is a strong one (i.e. malignant), it has spread (i.e. metastasized), and there is really no hope. Of course they are getting the best doctors and choosing all the best treatments, but the odds are poor and really it is just a matter of time.
Both of these men rejected my simple suggestions that would not have hurt anything to try, and could have helped. The stated reason? You have bladder cancer, but this is a different cancer, so nothing you say is applicable. The real reason? Both of them had accepted death as fait accompli, which is needless and dangerous, because, as it played out, both of the cancer patients became cancer victims and died a few months later.
 We have been trained (especially in America) to ONLY do
what the doctor says and hope for the best. I know a lot of doctors and
count some of them among my best and most faithful friends. They are
some really smart people. I also know that they are human beings -
trained in specialized skills to the exclusion of nearly all else. As
such doctors are quite valuable resources for the things that they know
about. We should pay attention to what doctors know and recommend, and
we should work together with them to defeat the cancer. Let me repeat
that for emphasis - WORK TO DEFEAT THE CANCER. This is step one. If you
cannot take this step, then you have already decided to die from cancer.
Anything you do after that is a simple matter of "just going through
the motions."
We have been trained (especially in America) to ONLY do
what the doctor says and hope for the best. I know a lot of doctors and
count some of them among my best and most faithful friends. They are
some really smart people. I also know that they are human beings -
trained in specialized skills to the exclusion of nearly all else. As
such doctors are quite valuable resources for the things that they know
about. We should pay attention to what doctors know and recommend, and
we should work together with them to defeat the cancer. Let me repeat
that for emphasis - WORK TO DEFEAT THE CANCER. This is step one. If you
cannot take this step, then you have already decided to die from cancer.
Anything you do after that is a simple matter of "just going through
the motions." In addition to the "doctor knows best" conditioning, we also accept that there is nothing else that can be done. Just surrender to the doctors and hope/pray for the best. And I heartily recommend most things that doctors will suggest. In addition, more can be done, and these extra things lie outside the areas of your doctors' collective training. Such things should NOT be viewed as ALTERNATIVE therapies. They are simply ADDITIONAL therapies. This whole nomenclature of "alternative medicine" has been a tremendous disservice. It's wrong-headed from every angle. It's not medicine, and it's not an alternative. These are reasonable and proper actions that can be taken in addition to taking conventional medical actions. Together they form a multi-pronged attack on the cancer and provide the basis for a healthy and longer life.
Attitude - the bottom line: If you believe cancer will kill you, it almost certainly will. If you believe that you can defeat the cancer, perhaps you can.
The goal is not to die FROM CANCER, which gives you the privilege to die from something else, hopefully much later in life. Perhaps something like a skydiving accident on your 100th birthday, having too much sex, or other happy pursuits.
 This brings us to Step 2 is a
combination of following the doctor's advice while educating yourself
and your support team, and adding to that medical advice everything that you can to
help your medical treatments to be successful. This last area is one
where your doctor has had zero formal training, so he or she probably
cannot help you, and most likely cannot even make an educated comment
about any of it. It is far more likely that the doctor will discourage such treatments, feeling that they could reduce the already long odds. There are a number of things to do, and I am doing many. Over time I believe the number one thing anyone can do for ANY type of cancer is to address "body chemistry." It is well known that cancer cells generate an acidic micro-environment which aids in their anaerobic metabolism and allows them to grow and expand at the margin. The blood and other fluid chemistry of ALL cancer patients tends towards the acidic (lower pH) ranges. Cancer causes acidity, and thrives in an acidic environment. How can we change the environment?
This brings us to Step 2 is a
combination of following the doctor's advice while educating yourself
and your support team, and adding to that medical advice everything that you can to
help your medical treatments to be successful. This last area is one
where your doctor has had zero formal training, so he or she probably
cannot help you, and most likely cannot even make an educated comment
about any of it. It is far more likely that the doctor will discourage such treatments, feeling that they could reduce the already long odds. There are a number of things to do, and I am doing many. Over time I believe the number one thing anyone can do for ANY type of cancer is to address "body chemistry." It is well known that cancer cells generate an acidic micro-environment which aids in their anaerobic metabolism and allows them to grow and expand at the margin. The blood and other fluid chemistry of ALL cancer patients tends towards the acidic (lower pH) ranges. Cancer causes acidity, and thrives in an acidic environment. How can we change the environment?First a few words about body pH. There is no such measure. Doctors routinely monitor blood pH, which the body regulates using its natural buffering system to within a very narrow range in healthy people, between 7.35 and 7.45 - slightly alkaline. (Neutral is 7.0 with values lower being acidic and higher being alkaline.) Arterial (oxygen-rich) blood tends to range higher (7.41) while venous blood tends more toward 7.36. For this reason most physicians scoff at the idea of alkalinity therapy to control or prevent cancer, because the bloodstream is already slightly alkaline, and it will not go above 7.45 - unless something else is seriously wrong with you. This line is reasoning is correct, as far as it goes. But as important as blood is, it comprises only about 10% of the total fluids in your body.
What is frequently and systematically overlooked by medical professionals is that the body is FULL of other fluids besides blood, and they are NOT as tightly buffered or regulated by natural systems. Besides urine these include saliva, lymph, spinal fluid, interstitial fluid, bile, aqueous and vitreous humors (in your eyeballs), endolymph (in your inner ear), and most importantly and most abundantly - cytosol - the fluid within each cell. Just to give you an idea, an average human male is about 60% water. If he weighs 190 pounds, then about 114 pounds are water. Most humans have about 5 liters of blood. A liter of water weighs about 2.2 pounds (and blood is a bit lighter than pure water). So only about 10-11 pounds of the 114 pounds of water is in your blood, which is pH controlled. That means there are at least 100 pounds (over 45 liters) of water-based fluids in your body other than blood, none of which are pH regulated like blood. The easiest one to measure pH on yourself is urine.

Measuring urine pH is potentially very helpful. Sadly, doctors will scoff at the idea, because urine naturally ranges widely in pH. As it should. But one must consider the function of urine. Its purpose is for elimination of things your body doesn't need, extracted from the bloodstream by the kidneys. While urine is mostly water, it can contain quite a few other things - over 3000 other things. The curious can find the entire list here: Urine Metabolome These things range from biological trash (broken cell pieces, enzymes, proteins, etc.) to salts, drugs, and environmental toxins. If you have too much of something present nearly anywhere in your body, it should ultimately show up in your urine. So if your urine is usually acid, that means that, somewhere in your body (probably many places) are running too acidic. This condition is common in almost all cancer patients, no matter what kind of cancer they have. If we could implement something that influences the body so that urine becomes routinely neutral or alkaline, this would imply that the alkaline capacity of the fluids in your body (other than blood) is maxed out - creating an environment that is less hospitable or even toxic to cancer growth.
I experimented for some weeks with diet, trying to modify food and drink intake to force urine to be less acid. It was a total failure, and was reproduced by other readers of the blog. You can see the details in this post.
You simply CANNOT influence body chemistry through diet. Even if you eat a kitchen sink full of broccoli and nothing else but distilled water daily, even this extreme diet cannot influence a very acidic body chemistry to any useful degree. A more dramatic input is required. What can you do?
Here is what I recommend: measure your urine pH for several days to determine if you have excess acidity. If so add one level teaspoon (that's TEAspoon, 5g, and NOT tablespoon) of baking soda to 8-12 oz or more of water and stir to dissolve.

Use a kitchen measure spoon, not a teaspoon from the flatware drawer. Drink the baking soda mixture ON AN EMPTY STOMACH (3-4 hours or more after your last meal) and wait at least 20 minutes afterward before eating any food (or drinking anything with food value, such as sugary drinks, jello, or soup). Continue to monitor your urine pH and adjust the timing and amount of baking soda so that you can keep your urine pH alkaline (7.0 or higher) for 24 hours or more. I have dialed in to one teaspoon, slightly heaped, every day - 7 days per week. (Don't try to double up the next day if you skip a day - this will probably result in a bout of diarrhea!) This is the simplest and easiest way to fight ANY type of cancer.
Be advised that the "alkalinity theory" of cancer treatment has been "debunked" in many places, most of which can be found with a web search. These debunkers make two primary errors - first they assume that blood pH is what we are talking about (even though blood only represents 10% of the fluids in your body), and second they assume that diet is the only method to implement alkalinity. Both assumptions are wrong. We are NOT trying to influence blood pH, nor are we trying to influence body chemistry through dietary changes! You will see BOTH of these incorrect presumptions embedded and implicit in all the literature against this approach. Here is a link to a pretty good one, and really he doesn't state that the approach won't work, merely that there is a lack of evidence to support a diet-based approach, and this is NOT a diet-based approach!
There are many other additional things you can do to fight cancer, in addition to what your doctors recommend, but having the right attitude and having the right body chemistry are the best place to start. Changing both of these will not hurt anything, and will actually help to win the battle against any type of cancer.
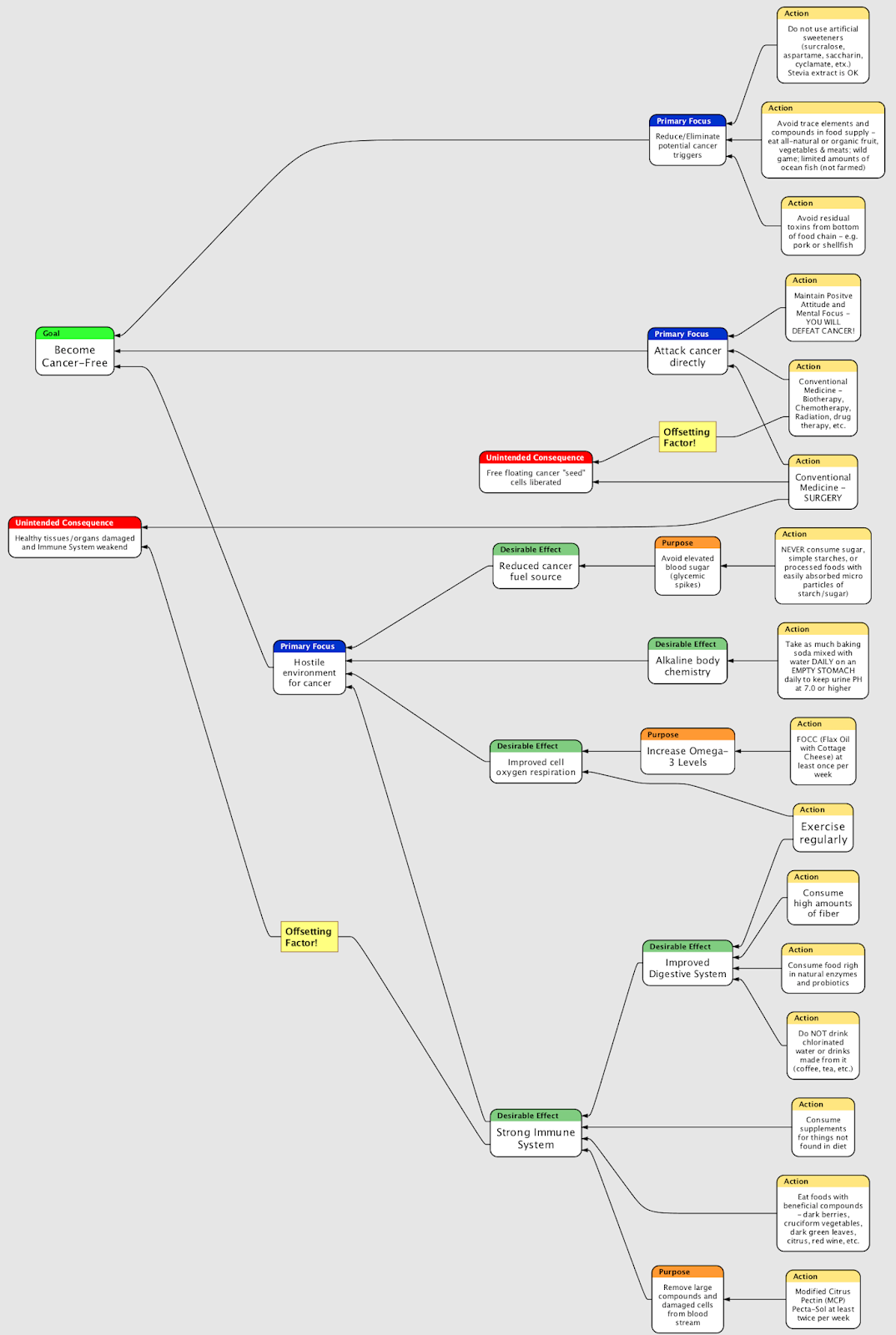
In 2008 I developed a logic diagram that breaks down what to do and why. I updated it in 2014, and again in 2019. You can see more rationale on the things I recommend and why in the updated post at this link: https://gotbladdercancer.blogspot.com/2009/10/dealing-with-any-type-of-cancer-what-to.html












{kind=link}
{kind=link}
{kind=link}