skip to main |
skip to sidebar
On Wednesday Kathryn and I drove down to Dr. Hopkins' office to get a debrief on the pathology results. My "friend" the Cat-in-Hat lady signed me in and checked my insurance. Dr. Hopkins does surgeries on Wednesdays, so we were scheduled to see the male Physician's Assistant (PA), Regan B. The Urology Clinic has four doctors, two PAs, some nurses, and a raft of administrative folks. They run patients through like a McDonald's at lunchtime in a normally efficient operation, so we had no issues with seeing the PA.  After a few short minutes a nurse led us to an exam room. "Can you give me a urine sample?" she asked. I could not, because I had just used the toilet in the waiting area. "No problem, just hop up on the exam table, and I'll be right back to do an ultrasound."
After a few short minutes a nurse led us to an exam room. "Can you give me a urine sample?" she asked. I could not, because I had just used the toilet in the waiting area. "No problem, just hop up on the exam table, and I'll be right back to do an ultrasound."
"Hold on a minute!" I interjected, "What do you think we are here for?" She flipped through my chart a bit and guessed, "Aren't you here for a BCG treatment?" I assured her that we were only here to TALK about BCG treatments, and I was not getting onto any table for anybody. She gave me a funny look, said, "OK," and left the room. A few minutes later Regan came in. He's a big, wide guy, young, in great shape, with coal black and curly hair. Apparently you have to be some sort of GQ model to work in this clinic. After talking for a few minutes, it became obvious that Regan also had not read my chart and had no earthly clue why we were there.  We informed him that we were there to get the pathology results and talk about the plan and schedule for BCG treatments, should they still be indicated. "The lab report isn't in here. When did you have surgery?" This was beyond frustrating. I kept trying to get him up to speed on my case, while he refused to listen with full attention. Kathryn finally insisted, "Can you at least call the lab or go look for the report?" Regan thought that was a good idea, clearly because Kathryn is much better looking than I am.
We informed him that we were there to get the pathology results and talk about the plan and schedule for BCG treatments, should they still be indicated. "The lab report isn't in here. When did you have surgery?" This was beyond frustrating. I kept trying to get him up to speed on my case, while he refused to listen with full attention. Kathryn finally insisted, "Can you at least call the lab or go look for the report?" Regan thought that was a good idea, clearly because Kathryn is much better looking than I am.
He returned a few minutes later. "Got it! Let's take a look." We had previously established that the probability of a surprise on the lab compared to Dr. Hopkins' visual inspection during surgery was unlikely, and the lab report bore that out. We learned a few new things:1) The previous cancer areas were free from regrowth, even at the microscopic level. 2) The new biopsies contained some muscle tissue, further supporting the non-invasive diagnosis. 3) The two new tumors removed were indeed "implants" as opposed to new, spontaneous growth. 4) The "implants" were non-invasive and G3, same as the original tumors they came from. 5) The "implants" grew pretty fast.
This was mostly good news, as far as we could tell. Regan added very little information, and we asked, "What's next?" He told us that I was indeed a candidate for BCG, which is also good news. We had about a dozen questions concerning the treatment - how soon could it start, how long could we wait at the outside, how much flexibility in treatment schedule, what action was taken during adverse reactions, and other questions. It turns out that Regan knew very few answers. He assured us there was a handout to give us that would tell us everything, though he had not read it himself. He also said he would have Dr. Hopkins call me the next day. I asked who gave the treatments. "Several of us here are trained to give them. I do some myself." I suggested that he might consider undergoing a treatment, so that he might in the process learn something about it. He laughed, but did not seem too keen on the idea.

We went to the front, gathered the famous handout, and requested a copy of my medical file to give to another doctor for a second opinion. I also had pre-written a "return to work" note per the instructions given by the company nurse. They put it in my file for Dr. Hopkins to sign. I asked how long it would take for the file, and they told me 2 weeks. "What if I get an appointment on Friday?" That was different, they would send it to another doctor right away, but the patient had to wait two weeks because of "legal stuff." This sounded very fishy to me, but at this point they hold all the cards. I explained that we had not learned what we came there for and were expecting a call from the doctor. They made another note to that effect. Kathryn drove me back to work, both of us stewing at the near-total waste of time.
Later that day I contacted the urological pathology department at the Huntsman Cancer Institute in Salt Lake, an independent operation from my clinic. Their doctors were both out on vacation, but the administrator there was very helpful. We discussed the logistics of a second opinion and the timing. Because of vacations they were a month out for appointments, but normally needed only a week's notice. He suggested waiting until my BCG sessions were complete before scheduling the second opinion appointment. He also thought the office attitude about my records was odd, but chalked it up to territorialism of the staff. He offered, "All the urology doctors in the valley here are friends, and they have no problem sharing information." While this was meant to be reassuring, it's less independence than I would have hoped for in a second opinion. I resolved to call Dr. Chuck again to see about an alternate.
The next morning I decided, based on previous experience, to make a pre-emptive strike. I called the urology clinic and explained that we needed more information, and someone should call us. They gated me to the nurses' voicemail, where I left a detailed message. By 4:30 nobody had called, so I called back. "We can't find your chart. Dr. Hopkins isn't in today." I said that Regan had the chart in his hand yesterday. "Regan isn't in today." I asked if she was really telling me there was no way to find anything out today. "I'll call you right back." I was skeptical. But 10 minutes later the phone rang, and it was Dr. Hopkins himself! "I thought you were out today," I said. He replied, "I had a root canal this morning, but decided to come in for an hour. Please overlook any slurring of my speech - I assure you it's not from drinking!" I had a load of questions, and started firing away. Dr. Hopkins patiently answered all of them, thoroughly. Here are the things I learned and/or verified:
Q) When is the earliest to start BCG?
A) I like to wait 4-6 weeks after surgery, for full healing. I don't want any BCG to have access through the un-healed lesions to get into your bloodstream. That's needless risk.
Q) When is the latest we should start?
A) No later than 8 weeks. We don't want to allow a spontaneous growth to start.
Q) When do you do the follow-up cytoscopic inspection? The handout says 6 weeks after BCG.
A) I like to wait a little longer. Sometimes there's residual inflammation that looks like something when it isn't. I shoot for 2-3 months, say 10 weeks after the last BCG treatment.
Q) If you find nothing?
A) Then 3 more weeks of BCG, and inspect again 3 months later.
Q) If you find growth, then we TURBT surgery again and re-baseline?
A) Not really. You have nothing now, verified by the pathology lab. Anything new will be spontaneous growth, and it tells us we have a very strong cancer that's behaving very aggressively. Further surgery risks spreading it, or risking that it becomes invasive. If we see anything at all, at your age we should consider more aggressive treatment at that point.
Q) Doesn't another TURBT buy more time?
A) I feel it drives more risk than the additional time is worth.
Q) So really the only more aggressive strategy is radical cystectomy, correct?
A) That's pretty much the only option.
Q) Ugh. I guess I should begin bracing myself for that eventuality.
A) You have a 50+% chance that BCG will work. If you have no growth for two years and then we see something small, we might consider doing TURBT again. We'll have to play it by ear.
Q) With the BCG, we have a latitude of plus or minus one day from week to week, correct?
A) I'd say so. I have even had patients skip a week to go on vacation. Since we don't really know the mechanism of how it works, we don't know if that's a problem or not. We tend to think in weekly increments, because that's how we live and work.
Q) If there is an adverse reaction, the classic approach is to skip a week, and the more current approach is to reduce the dosage. What's your recommended approach?
A) I usually skip a week, but if it happens, we can discuss other alternatives.
Q) Who actually does the BCG procedures?
A) I prefer to do them myself, for my patients.
Q) I read some research that if BCG is effective in eliminating the papillary cancer, you are at much greater risk for external bladder tumors. Is there a way to watch for those?
A) External tumors? Your ureters and kidneys have the same materials as the interior of the bladder, so if that's what they mean, it's standard procedure for us to do an x-ray screen of the kidneys and ureters every year or two.
NOTE: The doc is good - this is indeed what they meant - abstract HERE.
Q) On getting a second opinion, I guess the timing is any time from now until you do the next cytoscopy, as there really won't be anything new in the file until then?
A) That's correct. Getting a second opinion is a great practice, and I recommend it. So if you are on a business trip to Rochester in a month, you can get a second opinion then with no problems.
Q) On the three month follow-ups, how much leeway do we have? I'm trying to plan around a vacation to Mexico.
A) It's plus or minus two weeks, and we CAN accommodate your vacation!
Q) Thanks for your time. Lastly, I need a note for work. Who handles those for you?
A) I signed the note that you left in your file. All we need to do is fill in the dates for BCG treatment and send in the fax.
 Wow. That was a lot of good information in a short time! Let me give you the short version. I am currently CANCER-FREE!!!!! Let the rejoicing begin.! OK, we can stop rejoicing for a second - not clear of danger yet! We need to start BCG treatments ASAP after things heal, to get it going before any new growth can start. No new growth occurred in the last 6 weeks (implants don't count), so that 6-8 week window seems reasonable.
Wow. That was a lot of good information in a short time! Let me give you the short version. I am currently CANCER-FREE!!!!! Let the rejoicing begin.! OK, we can stop rejoicing for a second - not clear of danger yet! We need to start BCG treatments ASAP after things heal, to get it going before any new growth can start. No new growth occurred in the last 6 weeks (implants don't count), so that 6-8 week window seems reasonable. Starting BCG on July 2 would be exactly 6 weeks after surgery. That schedule would allow me to do a week-long business trip to D.C. and a week-long motorcycle rally in Taos in June! It does put a lot of limits on July, and it totally kills our plans to join BMWRS and his wife, brother, and friend on a motorcycle trip to Banff. I will personally suffer for this, as BMWRS will give me a ration of crap, and Kathryn will mention for the one-millionth time that she has not yet been to Lake Louise. Sigh. Gotta take the bad with the good, I suppose! Anyway, six weeks of BCG plus 10 weeks of recovery puts the cytoscope inspection on October 15, well after the Mexico trip and our 25th anniversary. The schedule is working out pretty well. So let the rejoicing begin again!!!!!
Starting BCG on July 2 would be exactly 6 weeks after surgery. That schedule would allow me to do a week-long business trip to D.C. and a week-long motorcycle rally in Taos in June! It does put a lot of limits on July, and it totally kills our plans to join BMWRS and his wife, brother, and friend on a motorcycle trip to Banff. I will personally suffer for this, as BMWRS will give me a ration of crap, and Kathryn will mention for the one-millionth time that she has not yet been to Lake Louise. Sigh. Gotta take the bad with the good, I suppose! Anyway, six weeks of BCG plus 10 weeks of recovery puts the cytoscope inspection on October 15, well after the Mexico trip and our 25th anniversary. The schedule is working out pretty well. So let the rejoicing begin again!!!!!
My recovery tactics started on Tuesday, the day before surgery. I met Frank and Bill from my church for a 6AM prayer breakfast. Bill is moving to Colorado soon, and may be getting married shortly after that, so we had plenty of topics for prayer besides my surgery. Normally I order a veggie omelet (egg whites, veggies, low-fat cheese, and salsa). But I decided to pound dietary fiber to make recovery easier, so I went with oatmeal, fruit, a Belgian waffle, and a side of bacon.  Robyn, our regular waitress, and my companions were all shocked to see my deviation from the norm, so I explained. Frank asked, "So what's the bacon for?" I replied, "Just to make me feel better now!" In keeping with my plans, Kathryn had packed me a high fiber lunch, also.
Robyn, our regular waitress, and my companions were all shocked to see my deviation from the norm, so I explained. Frank asked, "So what's the bacon for?" I replied, "Just to make me feel better now!" In keeping with my plans, Kathryn had packed me a high fiber lunch, also.
After lunch we had a quick staff meeting, and I was surprised by the team with a get-well card and an enormous gift basket from Great Harvest Bread. Even though I had not mentioned my fiber plans to anyone at work, these folks don't miss a trick - having read in a previous blog post that the best post-surgical meal is a couple of slices of whole-grain toast and jelly. They also had cookies and coffee cake for the meeting, all loaded with healthy soluble fiber. It was wonderful. Thanks!
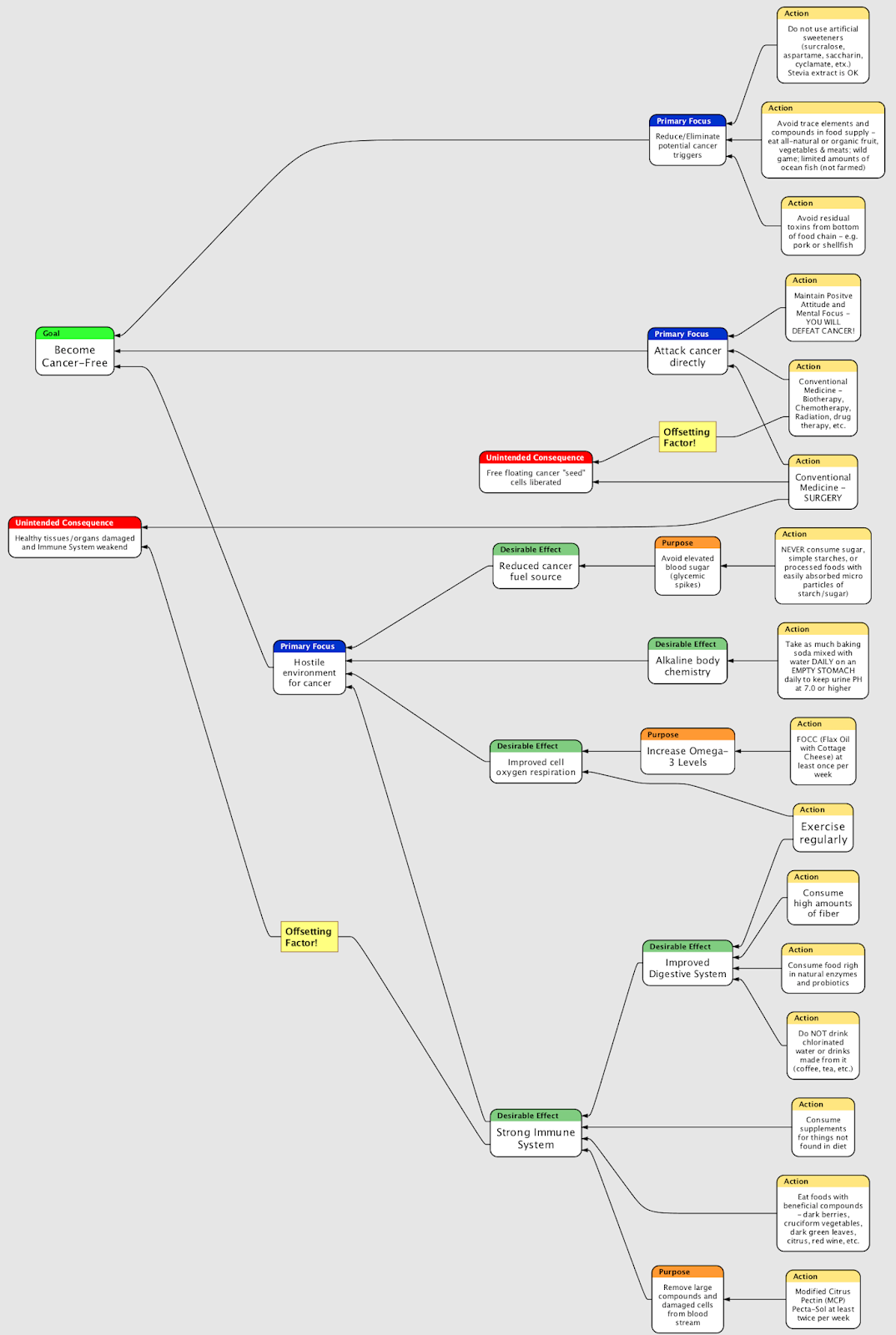
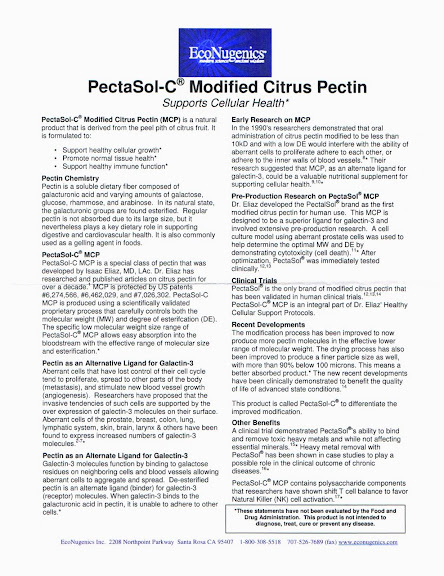
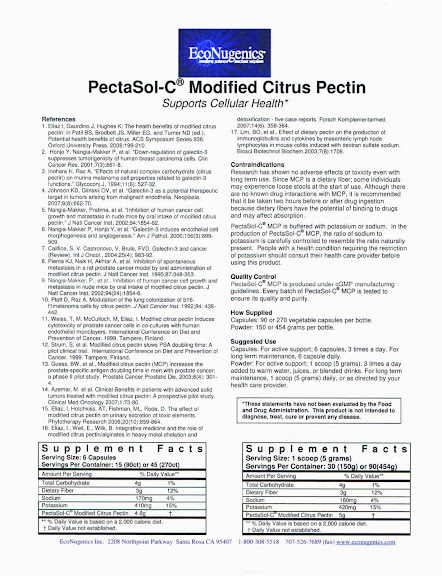
Dinner that night was meat loaf and veggies, to complete the fiber prep. It is worth noting that my parents are big fans of alternative medicine, and my mother had done a lot of research into alternative cancer cures. She found one that had a modicum of scientific testing (both animal and limited human trials) behind it, plus the fact that it was recommended as an adjunct to surgery and conventional medicine, and not a replacement. Modified Citrus Pectin (MCP) may have properties to ensnare free floating cancer cells, often released during surgery, and package them for elimination by the body's natural defenses. And, as a bonus, it's high in fiber! Dr. Chuck had suggested fiber supplements (9 grams/day) to help with my diverticulosis (a side diagnosis from Dr. Hopkins' read of the X-rays), and the daily dose of MCP has exactly 9 grams of fiber. Side effects are non-existent. So I've been taking PectaSolC three times daily for a while. It comes in powder form, totally tasteless, and has to be mixed with water, tea, or juice to consume. For an independent opinion on MCP, check out THIS LINK.
Upon arriving home after surgery on Wednesday, I immediately began pounding fluids in the desire to wash the burning residual from my bladder. I had received at least 4 liters of IV fluid during/after surgery, and had a few cups of water/ice chips after due to very dry mouth. It seemed that the output through the newly-installed (and still MUCH hated) tube was far less than the input. Had some Great Harvest whole wheat toast with jelly and a yummy honey/maple/hazelnut goop from my gift basket. About 10PM I began passing more than one liter per hour of fluid through the tube, keeping me busy and pretty sleep-free throughout the night. Had one Lortab at midnight to try to relax, but the constant need to empty the catheter reservoir outweighed all other activities!
It seems most surgical patients are released with a one-liter "leg bag" to get by with. Amazingly I had dealt with one for a full week last time, and it seemed no more than a minor nuisance. But my super-hydration this time made it nearly unbearable. I asked Kathryn to call our local doctor's office to see if we could get a larger bag to get me through the day and second night. "We couldn't just give you one, we have to check with the doctor," they said. Whatever.  A call to a recovery room nurse that attends our church was equally unfruitful, but a physical therapist from church made a few calls and suggested a couple of medical supply places. Kathryn ventured out and found that 2 liter bags were inexpensive, readily available, and unobtainable without a prescription! Freaking amazing - the proposed solution was that we call Dr. Hopkins office, wait for them to clear it with him, and then wait for them to fax the permission to the medical supply place. I told her to forget it and began mentally designing a milk jug solution. But Kathryn was undeterred in her pursuit of solutions to improve my discomfort, and she ultimately found a "back alley" supplier who provided a large bag for only $8.52. We were pleased to note the new bag was from C.R. Bard, a local medical device manufacturer where a friend of ours works. (Hi Vicki!) The new bag had several trick features and the large capacity provided sweet relief! To give you an idea, I emptied the very full one liter bag 5 times in the 3 hours she was gone.
A call to a recovery room nurse that attends our church was equally unfruitful, but a physical therapist from church made a few calls and suggested a couple of medical supply places. Kathryn ventured out and found that 2 liter bags were inexpensive, readily available, and unobtainable without a prescription! Freaking amazing - the proposed solution was that we call Dr. Hopkins office, wait for them to clear it with him, and then wait for them to fax the permission to the medical supply place. I told her to forget it and began mentally designing a milk jug solution. But Kathryn was undeterred in her pursuit of solutions to improve my discomfort, and she ultimately found a "back alley" supplier who provided a large bag for only $8.52. We were pleased to note the new bag was from C.R. Bard, a local medical device manufacturer where a friend of ours works. (Hi Vicki!) The new bag had several trick features and the large capacity provided sweet relief! To give you an idea, I emptied the very full one liter bag 5 times in the 3 hours she was gone.
Between trips to empty urine I noticed that my throat was still VERY sore from the day before. Not only that, there was a nasty dent in my inside, lower right gum area, and another cut on the inside of the right side of my upper lip. So it looks like Dr. Petersen and/or her med student, intern, or resident that day went to town on me with the hard, plastic airway. Senior docs often let students or interns observe or perform procedures to learn. I'm all for learning, but this secret stuff precludes feedback from patients. On Saturday afternoon three days later my gum injury still hurts. [Final report: this was a dental fistula, evidence that the tooth had been killed by the anesthesia, and necessitated my first and only root canal in what had been a perfectly healthy tooth with no fillings!] So for Dr. Petersen (or student) here's some feedback - YOU SUCK! And practice on somebody else next time!
Still no appetite, I had toast again for breakfast and dinner on Thursday. And still pounding fluids. With the improved reservoir situation I was able to sleep for a couple of 3 hour intervals on Thursday night, and was up at 7AM on Friday. Not feeling rested or refreshed, but looking forward to getting the hated tube out. Not fun for my loving wife, but accomplished without incident. Detailed description of this and other comedies for the non-squeamish are detailed on the backpage link referenced below. Still no appetite on Friday, but I forced oatmeal for breakfast, soup and toast for lunch, and a turkey pot pie for dinner. All with tons of fluid. Restarting both the normal urinary system and the gastrointestinal system at the same time on Friday was a bad call, also described on the backpages.  Suffice it to say that I could not go out in public or be more than 5 steps from the toilet all day Friday, but the situation improved slowly during the day.
Suffice it to say that I could not go out in public or be more than 5 steps from the toilet all day Friday, but the situation improved slowly during the day.
Friday night I was able to sleep six full hours at a stretch with no accidents. Got nine hours total sleep and feel almost 80% on Saturday morning - Happy 49th Birthday to me! Something that would have been a non-event now seems much more special to me now. Eager to reach 50 and beyond - no longer taking it all for granted. GI and urinary systems near normal now, and I can probably go out in public today. Appetite slowly returning. Planning for church attendance tomorrow. Stay tuned!
Backpage Link HERE - Not for the squeamish. Ranges from 5-7 on the gross-out scale where 10 is max gross-out!
Hello everybody! Thanks for your prayers, good thoughts, and support. This Surgery #2 should have been the same as Surgery #1, but there were a few odd differences to describe.
We were earlier in the schedule for this second surgery. I asked several folks how the sequencing was determined, and nobody really knew. Anyway, we were told to report to the hospital at 9AM for a 10:30AM surgery time. Departing at 8:50 put us at the tail end of the Salt Lake City rush hour.  Utah does not have LA traffic or Boston traffic, but there are a couple of natural bottlenecks (mountains in the way) that make it really slow during the classic morning/afternoon rush. Thank the Sierra Club for preventing additional or wider roads, adding to the time, cost and misery of any fix. And Utah weather in May is always entertaining. In the 90s Monday and Tuesday, today was 45, overcast, and rainy. We got to the hospital and checked in at 9:10.
Utah does not have LA traffic or Boston traffic, but there are a couple of natural bottlenecks (mountains in the way) that make it really slow during the classic morning/afternoon rush. Thank the Sierra Club for preventing additional or wider roads, adding to the time, cost and misery of any fix. And Utah weather in May is always entertaining. In the 90s Monday and Tuesday, today was 45, overcast, and rainy. We got to the hospital and checked in at 9:10.
In registration I played 20 questions got processed in. This time they did not require payment up front, which was good - they still owe me $26 from last time! We went to the Ambulatory Care Center, where they showed us to a semi-private cubby, similar to last time, but with much higher traffic in the hall and outside the window. We were very pleased to find that we had the same outpatient nurse again, the most excellent Vicki. I was gowned and temped and BPd and resting comfortably in no time. Used the hypnosis deep breathing relaxation technique from last time the night before and this morning, so my BP was pretty close to normal. Better relaxation and having been through it all just six weeks before combined to dramatically reduce the stress. Kathryn and I watched TLC network's "What Not to Wear" from 10-11, and I was wheeled upstairs at 11:15 - already they were 45 minutes late. Brad, the orderly that took me up, was an enormous guy - like a college football lineman. He and I joked about how he was the guy they used for troublemakers and I must be one.
After 15 minutes or so Michelle, the pre-op nurse came in and introduced herself. A petite blonde, about 50, she was there to check paperwork and start the IV. I gave her the standard warning about being a "hard stick," so she took her time and made sure everything went smoothly - and so it did. We talked for a few minutes about a variety of topics - Michelle has a great, reassuring bedside manner. I asked why I didn't have a pre-op nurse before, and she said sometimes they move folks in and out before she can finish rounds. She moved on to work the others and left me alone for what seemed like half an hour. You are surrounded by curtains and can see nothing outside. With no watch, reading materials, TV, Blackberry, or other toys, there was absolutely nothing to do at all, except to eavesdrop. There were only two other patients in pre-op, both women, both having some female parts removed. The lady next to me was very nervous, and Michelle spent a lot of time reassuring her. I could tell that it helped a lot.
I had been told that my anesthesiologist would be Dr. Petersen this time. She came in and grabbed the gurney, taking me over to the operating room. Older than Michelle and strictly business, she told me all the standard stuff about breathing tubes, IV, etc. I asked if we would do a countdown, because we didn't last time. "We can if you want," she replied, smiling for the first time. "Just surprise me." I answered. She left me in the hallway - something to do with the OR not being ready. Several people passed by, going about their business, and most ignored me - not making eye contact. This is pretty normal behavior - surgeons and staff need to emotionally distance themselves from patients to do their best work.  Keith, the OR nurse, came by for 20 questions and introduced himself - he was the same guy I had before. Dr. Hopkins also came by, fresh from two weeks in Paris. He was still in sticker shock at the unfavorable exchange rate ($1.55 per Euro) and high prices, but admitted the food was amazing. He also reassured me he would take a different approach on local paralysis to guarantee no repeat of the unpleasant events last time. A few minutes later I was on the table. Keith and another nurse joked and got me situated - apparently we were waiting for Dr. Petersen. She and Dr. Hopkins were still working with the previous patient and family in recovery - not a very good sign, for him. I was pretty relaxed and happy, and Dr. Petersen came in and pumped something into the IV that made me feel warm.
Keith, the OR nurse, came by for 20 questions and introduced himself - he was the same guy I had before. Dr. Hopkins also came by, fresh from two weeks in Paris. He was still in sticker shock at the unfavorable exchange rate ($1.55 per Euro) and high prices, but admitted the food was amazing. He also reassured me he would take a different approach on local paralysis to guarantee no repeat of the unpleasant events last time. A few minutes later I was on the table. Keith and another nurse joked and got me situated - apparently we were waiting for Dr. Petersen. She and Dr. Hopkins were still working with the previous patient and family in recovery - not a very good sign, for him. I was pretty relaxed and happy, and Dr. Petersen came in and pumped something into the IV that made me feel warm.
Two seconds later I was scooting into a bed in the recovery room. Dr. Hopkins was there and spoke to me about prognosis - no visible regrowth in the area, but two new very small (1mm) growths removed. He called them "implants" and said they were probably a result of not doing chemo last time. We were doing it this time, and I could feel the burning. This was a good sign, as it meant no bladder puncture this time! They were using Mytomycin and there was a pretty strong urge to pee, even though the catheter was in, because it was clamped off to hold in the chemo treatment. I talked with Millie, the recovery room nurse, who was the same one who had taken care of me last time. She said I looked familiar, and looked up on the computer to be sure. Indeed same as last time. She did not remember my getting cranky with her last time, so that was good. Dr. Hopkins came in again and showed me photos of the two "implants" he removed. (No snickering - you in the back. You know who you are!) He asked if I remembered his first visit, and this time I did..jpg)
Millie and I talked a bit. She noted that my BP was too high and my heart rate was irregular, and she said I was not behaving. I assured her once she unclamped the tube that it would all dial in. She checked her watch and looked concerned. Grabbing Dr. Petersen for a consult, the advice was to wait. Millie took mercy and opened the floodgates 5 minutes early (55 min instead of the full hour). Soon my vitals were back in line and I was "behaving."
Ten minutes later I was back with Kathryn and nurse Vicki in Ambulatory Care. We were all happy, feeling good, and ready to roll. But I had more IV to absorb, and other vitals to be monitored. Best news of all was that I could get the hated tube out on Friday, and it was not necessary to go to the Doc's office to do it. Kathryn was not eager to become a nurse, but she's tough and would do well when the time came. I asked if Friday meant 12:01AM, and they told me more like 8AM. Oh, well... And Kyle, the helpful CNA, had come on duty, and I thanked him for his very practical help last time. So we made a day of it, hitting the tail end of rush hour back North, and Kathryn battled the post-work crowd in Target to get the prescriptions filled. Got home at 6:30PM and began the comedy of post-operative recovery, to be detailed in the next blog entry.
There's no medical news to report, as we still are awaiting biopsy surgery on Wednesday, May 21. I added a meter to the page, and I can now see that a lot of you are checking for updates. So I thought I should fill in the gaps since my perfect day on May 5. The very next day I left late in the afternoon for Los Angeles. The Salt Lake City Airport has re-done their parking lot from very convenient to enormous and inconvenient. A 5 minute bus ride has been replaced with a 15-20 minute ride. A lot of us locals boycott the parking lot bus entirely and opt to walk to the terminal. There's one small area in the lot where this is possible, and spaces are scarce. I happened to drive by just as someone pulled out - great to be Irish and lucky! The trudge through the lot and parking garage to security is a pretty long one (albeit NOT 15 minutes), and the trudge from security to the commuter plane terminal is nearly as long.  This trip was a one-night deal, so I had a light bag and a heavy laptop/briefcase - both carried by hand and not checked. I had no abdominal discomfort, which was good. Got to LA , procured rental car (Mercury Grand Marquis - no satellite radio), and hit the hotel (Staybridge Torrance) without incident.
This trip was a one-night deal, so I had a light bag and a heavy laptop/briefcase - both carried by hand and not checked. I had no abdominal discomfort, which was good. Got to LA , procured rental car (Mercury Grand Marquis - no satellite radio), and hit the hotel (Staybridge Torrance) without incident.
Had a phenomenal dinner at Kappo Seafood (closed permanently in 2010), and hit the sack early. Also got up early, had breakfast at the hotel (complimentary and good), and wasted 20 minutes trying to check in and get my boarding pass for the evening's 7PM departure. The Delta website was egregiously slow and finally allowed check-in, but it refused several attempts to print the boarding pass - as it has done the past 3 times. You'd think I would learn. Now running late, I grabbed baggage, checked out, and raced to the facility. I wanted to arrive at 7:30 for the 8AM meeting to strategize with the organizers on how to facilitate. I made it, but in my rush forgot my Blackberry in the room. Nobody was there, and the room was locked.
The admins in the area assured me everyone would be there at 8, and asked me to wait. With folks coming in from all over the country, I wondered how they could be so sure. I called the hotel and they made a note to look for the Blackberry. 15 minutes later, still nobody there. I decided to go back for my lost toy. The admins were concerned, as they were sure all would be present at 8. Since they had not bothered to come early and meet as we'd agreed, I felt my obligation to be on time was waived. "They can start without me," I declared, and left.
Got back at 8:30 and went in to the admin area to get my laptop case. One asked me if I was associated with acronym I was unfamiliar with. After further discussion, we determined that I had not showed up half an hour early, but 23.5 hours late! THE MEETING WAS YESTERDAY! In 25 years I have never (unintentionally) missed a meeting. Until now. There are no words to capture how I felt, but Homer Simpson gets close...
I apologized to the meeting organizer, with whom the now friendly admins connected me via phone, and I tried to make lemonade from my lemons. I drove to another building at that site to meet a co-worker on another project, but she was out sick. Called back to Utah to see if they needed anything done in LA - not really. I eventually bagged it, returned to LAX for an earlier flight, got home a 3PM, and crashed. I debated whether to relate this embarrassing story to all of you, but the humor quotient is too high to leave it out. Maybe someday I will be able to laugh about it, too! In the interest of saying something positive in all circumstances, I will note that the perfect day described in the last update would not have been possible had I been on time for the meeting!
Rest of the workweek was blissfully routine - or as routine as our never-ending panoply of odd tasks can be in process improvement. Weekend was nice, and Saturday found me doing spring cleaning in my home office, filling the garbage can and shredder bin both! On Sunday after church I spent a couple of hours temporarily wiring in my Nuvi GPS and new XM Xpress RC radio into the bike, and took it out into the boonies for a 75 mile shakedown cruise. Even on bad mountain roads nothing shook loose, so both locations and mounting arrangements are candidates for permanent wiring - later. I paused in a deserted state park to enjoy the sight and sound of a rushing creek, swollen with this year's ample snowmelt runoff.
This creek is normally almost dry, but you can see from the short film clip that it's petty active right now! As I mentioned, nothing refreshes like a brisk motorcycle ride, and the world started looking pretty good again, despite the cloudy overcast.
The workweek was unusual - my company had sponsored a major process improvement symposium at a local university. Most of our small group attended, and my boss gave two really good presentations. We heard a lot of new things from folks who were pioneering new and cutting-edge improvement ideas and tools. Back to our normal chaos on Friday. Weekend looks good with a church group dinner on Saturday and a wine dinner on Sunday. I am researching how and where to get a second opinion on diagnosis and recommended treatment this weekend, which I am told is the normal and proper thing to do. Any recommendations will be welcome. We are still awaiting surgery next Wednesday, and new lab results the following week after Memorial Day. Next update should be towards the end of next week!
Due to a panoply of chores on Saturday, including updating, editing, and beautifying this blog (which doesn't write itself) and a raft of church and social engagements on Sunday, another weekend has passed where I didn't ride the bike. Checking the  meetings on my calendar, I decided it would be possible to take Monday afternoon off and go for a ride!
meetings on my calendar, I decided it would be possible to take Monday afternoon off and go for a ride!
Every morning when I wake up, before I get out of bed, I say a little prayer. It always starts the same way, "Dear Lord, thank you for this day. It is a good day." And then I go on to whatever is on my mind, and often ask for mercy for Lisa S. who is recovering from massive surgery, radiation, and chemo in a situation much worse than my own. So started this Monday. After a quick shave and a shower, nice breakfast and I was off to work! Except when I got into my classic 1987 Toyota 4Runner, it wouldn't start - dead as roadkill. This was very odd since we had used the truck all weekend and had returned from dinner near midnight the night before. It was pitch dark, so if I had left lights on or failed to close the door, it would have been easily seen. Got the Pilot and it jumpstarted easily. Ran for several minutes and turned it off. Dead again. Jumpstarted again and ran for half an hour. Called my friend Rusty - if there's anything he doesn't know about Toyotas it's not worth knowing. He said the alternator and regulator were combined into one unit on my truck, or it could be a battery. The battery was pretty new, and there had been no warning that it might fail. I feared it might be the much more expensive alternative!
This situation had tremendous potential to be annoying, since I had just spent about $1000 on general maintenance to get the inspection passed. Nothing big - just a lot of routine things needed doing at once - muffler, belts, steering hose, rear brakes, rear seals, wheel bearings, etc. The truck has over 250,000 miles on it, and it has served us well. I went to the place that had done the belts, radiator, and hose, and they ran a charging system check for me. Five minutes later we knew it was the battery. GREAT NEWS! How much did I owe? No charge! MORE GREAT NEWS! I decided to go to Sam's Club, where I purchased the battery, and see if maybe I could get a credit for the old one. Drove to the tire center and parked outside. Waved through the window to get their attention - they are open only to business members before 10 AM, and I am one, but they don't get much activity this early. I explained that I needed a battery, but did not want to park, since the truck would then not start. They cheerfully pulled it into the garage for me, and found a new battery. Although I had purchased the old one at a different location, they were able to find me in the computer. Purchase was May, 2005. Three years ago. They also found that my battery had a three year full replacement guarantee. So my new battery, installed, was free. And I now have another three years of warranty! EVEN MORE GREAT NEWS!
I was only a couple of hours late to work, and didn't miss any meetings. Came home for a late lunch, geared up, and went out and pre-flighted the bike. It was in perfect condition and ready to roll. So out we went. I mentioned in an earlier entry that motorcycling requires tremendous concentration to ride safely, and is an ideal hobby for my personality type. I had been getting irritable of late over small things. When I was young I found sports to be a great release. But with age and injuries all I have left is riding the bike. The cognitive part of the brain must be fully engaged, and such an exercise really purges the spirit like a good workout can purify your muscles. A friend captured it well:
On the open range the road, the landscape, and the machine all provide an experience that is for me soul centering. The rhythm of the ride is at once calming, reassuring. It is rarely achieved until more than a hundred miles have been traveled. This period of lonely introspection and intense observation yields a sense of appreciation and perspective of life that I've never experienced in any other endeavor. It is like meditation, but perhaps a little more like worship. The intensity of concentration required is at once enormous and yet completely liberating. - W.C.H. June 1, 1999
I believe the desire to ride a motorcycle is in your genetic makeup. I wanted to own one and ride one from the very first time I saw one as a little kid. Like musicians that must play music and writers that must write, bikers must ride.  Or they get physically and emotionally ill. This often happens in the winter, and my group jokingly refers to it as "Motorcyclene withdrawal." Motorcyclene is a mythical endorphin that is released to cause joy when riding. On this afternoon, temperatures in the mid 7os, sky clear an blue with some decorative white, puffy clouds, and surrounded by mountains covered with snow, the ride was PERFECT!
Or they get physically and emotionally ill. This often happens in the winter, and my group jokingly refers to it as "Motorcyclene withdrawal." Motorcyclene is a mythical endorphin that is released to cause joy when riding. On this afternoon, temperatures in the mid 7os, sky clear an blue with some decorative white, puffy clouds, and surrounded by mountains covered with snow, the ride was PERFECT!
I had not ridden since January, so I took it easy on the speed (for me), and kept it under 100MPH (mostly). It was a fine experience. Life improved minute by minute. Unlike WCH above I am not on the open road, but on twisty back roads covered in winter silt, my cognitive mind is busy noting and avoiding all the potential hazards, there is no time for introspection, and that's a good thing! I rode to a knoll overlooking the railroad tracks and popped open a bottle of water. Eastbound train traffic was thick, and a long coal-filled train passed me by. I could not resist the urge to place a couple of coins on the track and wait for the next train. A few minutes later a chemical tank train came by and obliged.  I had 11 cents change from mailing my passport renewal, so that dime and penny were sacrificed to my boyish urge. You can barely make out the penny's design from the oxidation. The dime is completely blank, and you can barely see the knurled edge. While all this was great fun, I decided to check my messages. There was one from the Urology Clinic, with a question about my surgery date.
I had 11 cents change from mailing my passport renewal, so that dime and penny were sacrificed to my boyish urge. You can barely make out the penny's design from the oxidation. The dime is completely blank, and you can barely see the knurled edge. While all this was great fun, I decided to check my messages. There was one from the Urology Clinic, with a question about my surgery date.
Hmm. I tried calling out, but could not get a good signal at that remote site. Guess they can wait! Finished the water and gave some back to the environment. Rode down to the top of Echo Reservoir dam and parked illegally while I made the call back. During my last visit the surgical coordinator had taken the afternoon off for a new grandbaby. The backup person knew the paperwork and procedure, but she forgot to check Dr. Hopkins' vacation schedule. Turns out he is on vacation this week and next, so we need to delay from May 14 to May 21. I asked if that meant the doc would be relaxed, rested, and refreshed for me and was assured that would be the case. So we are rescheduled for a week later. What does this mean? Just one more week of feeling good, eating well, doing work and chores, and riding the motorcycle. Sure, the prognosis would be delayed, but this seemed to be a small thing compared to all the benefits. And really I was not prepared for another surgery so soon. The new schedule makes it 6 weeks later instead of 5, and I think it's ALL GOOD NEWS!
I called my wife with the update. She was annoyed at the delay, but accepted my interpretation of it. I rode some more, and came home mentally and physically exhausted - in a good way. After a nice dinner and some TV, I went to bed and SLEPT LIKE A ROCK for the first time in weeks.
So even though the start of the day seemed to be a problem, we see that it ended up as A PERFECT DAY!
Welcome to the Bladder Cancer Weblog!!! For some of you it will be the first time around, so let me give you a quick tour.  The photo at the top is a gorgeous Ferrari Fi-430. It does not belong to me, but to "new age guy" mentioned in earlier blog entries. He was kind enough to let me drive it, and the car and I bonded instantly. I think it misses me, too! On the left we have my CURRENT STATUS, leading off with a link to this post for first timers and a link to the FIRST POST IN THE BLOG so you can read the story from the beginning to the current period. Below that is a short summary section of what's transpired do far. It's there to give fast info to those who don't care for my verbose style. Just below that are POST LABELS so those of you who have found this blog via a topic search can find all the blog posts related to a specific topic by clicking on it. Below that are some useful reference links.
Then there are a couple of mechanisms to subscribe to the blog updates,
either via reader or via email notice. Below this are recommended
books, followed by details of my medical history - provided for any who
might be in a similar situation. At the bottom of the left column are
other things that may interest or amuse you.
Below that is a short medical history and below that are supplemental links to specific topics of interest to anybody with bladder cancer.
In
the large area center and right (where you are reading this now) is
where the blog entries go, newest on top. You can also find the entries
listed in chronological order on the left side in the BLOG ARCHIVE, near
the bottom. So those so inclined can read the whole story from the
beginning! Or jump to any title that looks interesting. Click on any
entry's title and it will take you directly there.
The photo at the top is a gorgeous Ferrari Fi-430. It does not belong to me, but to "new age guy" mentioned in earlier blog entries. He was kind enough to let me drive it, and the car and I bonded instantly. I think it misses me, too! On the left we have my CURRENT STATUS, leading off with a link to this post for first timers and a link to the FIRST POST IN THE BLOG so you can read the story from the beginning to the current period. Below that is a short summary section of what's transpired do far. It's there to give fast info to those who don't care for my verbose style. Just below that are POST LABELS so those of you who have found this blog via a topic search can find all the blog posts related to a specific topic by clicking on it. Below that are some useful reference links.
Then there are a couple of mechanisms to subscribe to the blog updates,
either via reader or via email notice. Below this are recommended
books, followed by details of my medical history - provided for any who
might be in a similar situation. At the bottom of the left column are
other things that may interest or amuse you.
Below that is a short medical history and below that are supplemental links to specific topics of interest to anybody with bladder cancer.
In
the large area center and right (where you are reading this now) is
where the blog entries go, newest on top. You can also find the entries
listed in chronological order on the left side in the BLOG ARCHIVE, near
the bottom. So those so inclined can read the whole story from the
beginning! Or jump to any title that looks interesting. Click on any
entry's title and it will take you directly there.
The blog entries describe the details of the main story of my battle with bladder cancer. The gory parts are NOT described there in detail, so the reading is safe for all but the most squeamish. Instead, those graphic details are hidden behind links with appropriate warnings - often with an estimate of how stomach-churning such details might be. Click on those at your own risk! At the bottom of each blog entry there is a link that counts the number of comments. Click on it to add your own comments as you see fit. This week's entry describes the thoughts and process I went through to let folks know about my situation. It's not easy news to communicate, and I appreciate all of you who are interested to read along as things progress...
One thing that's been a major concern is how to break the news to folks. There is an inner circle of friends and family that were informed of every step. The middle circle, concerned folks at church and at work, found out after the diagnosis on March 31. Just disappearing for surgery without explanation would have been rude.  You can take the "minor surgery - couple of days - no big thing" route, but that plan creates tracking problems - who have you told and who not? And some people want to know only the minimum fact set, some want the main story, and some really get into the graphic details. It's impossible to predict who is in what list. Sometimes it's men that want the details, but often it's women. In many ways they can be tougher and less squeamish than men.
You can take the "minor surgery - couple of days - no big thing" route, but that plan creates tracking problems - who have you told and who not? And some people want to know only the minimum fact set, some want the main story, and some really get into the graphic details. It's impossible to predict who is in what list. Sometimes it's men that want the details, but often it's women. In many ways they can be tougher and less squeamish than men.
Public law, the medical community, and the human resource department of my major corporation are all set up to keep everything private and confidential. That's why you have to sign all those HIPAA forms (Health Insurance Portability and Accountability Act of 1996) at every doctor's office and hospital - to give the docs permission to talk to each other about treating you. Lots of folks do prefer to keep bad news private, so the system is good for them. I can't see handling the added complexity of tracking lists of "who knows what," so I decided to let folks know in an orderly fashion, and ultimately it would just become general knowledge in the circles where I function - church, work, and the motorcycling community. I talked to our HR manager, who was very sympathetic. She was pleased to hear about a medical problem that did not seem to be leading to a tragic ending - she gets all of those. And she's dealt with severe illness in her own home. I asked her to let her staff know so they could help keep rumors in check. Soon the building might be buzzing with "Steve's dying of cancer" misinformation, and I want the official spokespeople and my close friends to have the details to rebut such foolishness.
So how to inform those in the outer circle? I had some practice breaking the news already, and it often did not go well. I decided to call a buddy who had been around the block - he had shared some graphic details of his issues with an episode of priapism (graphic content), so I figured he'd be tough enough to take it well. I was wrong about that. He'd lost a number of good friends in the last couple of years, and he mentally leaped to the wrong scenario. We talked for over an hour while his dinner got cold, and ultimately arrived at the communication plan that was outlined in the last blog entry. Basically lead in with NON LIFE THREATENING, drop the "c-word bomb" and be upbeat about the range of probable outcomes, and end with MY LIFE IS NOT IN DANGER. I tried this approach in general a number of times in face-to-face meetings with folks where that type of meeting was possible. Results were somewhat mixed. So I spent the last few days crafting an email that would elaborate on that structure. While driving home from the airport on Thursday I called a friend who had a question about purchasing a new mattress. We had purchased and returned one from Costco, and then purchased a different one that we like a lot. We discussed pros and cons for a bit, and he asked if we were attending an upcoming dinner party. When I replied in the negative due to upcoming surgery, I realized that he had not heard the news. So I tried a verbal version. By his reaction, I guess it still needs work. He later sent an email after reading this blog, which he found to be "inspirational." I will try not to let it go to my head!
On Friday and Saturday I started emailing to the outer circle folks. I sent each family a separate message, based on the following framework, personalizing each one a bit:
Subject: Medical News Blues<- span="">
I have found out that I have a medical condition that is NOT LIFE THREATENING, but it sounds bad. I was diagnosed with bladder cancer. If you are going to get a cancer, this is the one to pick - it's very treatable and the prognosis is good. While my life is not at risk, there is still a battle for my bladder. If they can stay ahead of it (kill it faster than it grows), eventually I will just need annual checkups to make sure it's gone. If not, they can build me a new bladder out of spare parts in the abdomen. So the worst case is a major surgery, and the best case is a nuisance. So while MY LIFE IS NOT IN DANGER from this, your prayers and good thoughts would be appreciated.
Sorry for the bombshell. No good way to tell folks about it. I am upbeat and optimistic and feel fine. So you should be too!
I have started a blog to share details (and the gross stuff is hidden behind links, so you don't have to see that unless you ask for it). I will send out a big email distribution whenever I update it. Please take a minute and check it out. It's supposed to poke fun at all the ridiculous things that one goes through. Feel free to leave wisecracks and other encouragement using the comments feature on the blog.
http://gotbladdercancer.blogspot.com/
Later,
SK
This format seems to be working quite well. It gives people time to absorb and react, and/or do a little research and come to terms in private. Not so with a phone call or face-to-face. I have found that Christians in general seem to handle the news better than others. Feel free to borrow the format should you need to break bad news to loved ones!
Not so with a phone call or face-to-face. I have found that Christians in general seem to handle the news better than others. Feel free to borrow the format should you need to break bad news to loved ones!
For the vast majority of folks who are e-savvy and use email and the internet, this approach combined with the blog should work well to keep everyone up to date. I realize that folks can subscribe to updates, but I plan to send email reminders anyway. The list is over 50 folks for the regular updates. The problem is for the few (about 10%) who won't use email or read the internet. I will phone them using the basic structure of the email. If they won't read the blog, I'm not sure how to keep them informed. Would be interested in any ideas you readers have!
Use the comments function below. You click on the "x comments" and it will take you to another page, where you can crack wise or leave other gems of wisdom!
 After a few short minutes a nurse led us to an exam room. "Can you give me a urine sample?" she asked. I could not, because I had just used the toilet in the waiting area. "No problem, just hop up on the exam table, and I'll be right back to do an ultrasound."
After a few short minutes a nurse led us to an exam room. "Can you give me a urine sample?" she asked. I could not, because I had just used the toilet in the waiting area. "No problem, just hop up on the exam table, and I'll be right back to do an ultrasound." We informed him that we were there to get the pathology results and talk about the plan and schedule for BCG treatments, should they still be indicated. "The lab report isn't in here. When did you have surgery?" This was beyond frustrating. I kept trying to get him up to speed on my case, while he refused to listen with full attention. Kathryn finally insisted, "Can you at least call the lab or go look for the report?" Regan thought that was a good idea, clearly because Kathryn is much better looking than I am.
We informed him that we were there to get the pathology results and talk about the plan and schedule for BCG treatments, should they still be indicated. "The lab report isn't in here. When did you have surgery?" This was beyond frustrating. I kept trying to get him up to speed on my case, while he refused to listen with full attention. Kathryn finally insisted, "Can you at least call the lab or go look for the report?" Regan thought that was a good idea, clearly because Kathryn is much better looking than I am.
 Wow. That was a lot of good information in a short time! Let me give you the short version. I am currently CANCER-FREE!!!!! Let the rejoicing begin.! OK, we can stop rejoicing for a second - not clear of danger yet! We need to start BCG treatments ASAP after things heal, to get it going before any new growth can start. No new growth occurred in the last 6 weeks (implants don't count), so that 6-8 week window seems reasonable.
Wow. That was a lot of good information in a short time! Let me give you the short version. I am currently CANCER-FREE!!!!! Let the rejoicing begin.! OK, we can stop rejoicing for a second - not clear of danger yet! We need to start BCG treatments ASAP after things heal, to get it going before any new growth can start. No new growth occurred in the last 6 weeks (implants don't count), so that 6-8 week window seems reasonable. Starting BCG on July 2 would be exactly 6 weeks after surgery. That schedule would allow me to do a week-long business trip to D.C. and a week-long motorcycle rally in Taos in June! It does put a lot of limits on July, and it totally kills our plans to join BMWRS and his wife, brother, and friend on a motorcycle trip to Banff. I will personally suffer for this, as BMWRS will give me a ration of crap, and Kathryn will mention for the one-millionth time that she has not yet been to Lake Louise. Sigh. Gotta take the bad with the good, I suppose! Anyway, six weeks of BCG plus 10 weeks of recovery puts the cytoscope inspection on October 15, well after the Mexico trip and our 25th anniversary. The schedule is working out pretty well. So let the rejoicing begin again!!!!!
Starting BCG on July 2 would be exactly 6 weeks after surgery. That schedule would allow me to do a week-long business trip to D.C. and a week-long motorcycle rally in Taos in June! It does put a lot of limits on July, and it totally kills our plans to join BMWRS and his wife, brother, and friend on a motorcycle trip to Banff. I will personally suffer for this, as BMWRS will give me a ration of crap, and Kathryn will mention for the one-millionth time that she has not yet been to Lake Louise. Sigh. Gotta take the bad with the good, I suppose! Anyway, six weeks of BCG plus 10 weeks of recovery puts the cytoscope inspection on October 15, well after the Mexico trip and our 25th anniversary. The schedule is working out pretty well. So let the rejoicing begin again!!!!!
















{kind=link}
{kind=link}
{kind=link}